

Current evaluation of amenorrhea: a committee opinion
Download a PDF of this documentAmenorrhea is the absence or abnormal cessation of menses (1). Primary and secondary amenorrhea describe the occurrence of amenorrhea before and after menarche, respectively. Most of the causes of primary and secondary amenorrhea are similar. Timing of the evaluation of primary amenorrhea recognizes the trend to earlier age at menarche. It is therefore indicated when there has been a failure to menstruate by the age of 15 in the presence of normal secondary sexual development (2 standard deviations above the mean of 13 years), or within 5 years after breast development if that occurs before the age of 10 (2). Failure to initiate breast development by the age of 13 (2 standard deviations above the mean of 10 years) also requires investigation (2). In women with regular menstrual cycles, a delay of menses for as little as 1 week may require the exclusion of pregnancy. Secondary amenorrhea, defined as the absence of menses for >3 months in girls or women who previously had regular menstrual cycles or 6 months in girls or women who had irregular menses, requires investigation.
CAUSES OF AMENORRHEA
The prevalence of amenorrhea not because of pregnancy, lactation, or menopause is approximately 3%–4% (3, 4). Requirements for normal menstrual function include four distinct functional and structural components: the hypothalamus, the anterior pituitary, the ovaries, and the genital outflow tract (5). Pathologies in any of these components can lead to amenorrhea.
Although the list of potential causes of amenorrhea is long (Table 1), most cases are accounted for by six conditions: polycystic ovary syndrome (PCOS), hyperprolactinemia, thyroid dysfunction, hypogonadotropic and hypergonadotropic hypogonadism, and anatomic abnormalities. Other causes are less frequently encountered in a typical reproductive medicine practice. In specialized referral centers, approximately 5–20 patients per year were seen with primary amenorrhea annually (6–8).
Amenorrhea may also occur with sexual ambiguity or virilization, but usually, in these cases, amenorrhea is not the primary complaint. Sexual ambiguity or virilization should be evaluated as separate disorders, being mindful that amenorrhea is an important component of their presentation (9, 10).
Table 1. Causes of primary amenorrhea (7,22,23).
| Primary amenorrhea | Aorixunate frequency | |
| Hypothalamus | Constitutional delay Functional hypothalamic amenorrhea Isolated GnRH Deficiency Inflammatory or infiltrative disease Infection Tumor Radiation Traumatic brain injury |
10%–21% |
| Anterior pituitary | Hyperprolactinemia Pituitary tumors Inflammatory and infiltrative disorders Radiation/surgery Infection GnRH receptor mutation |
1%–4% |
| Ovary | Primary ovarian insufficiency Gonadal dysgenesis Gonadal agenesis Polycystic ovary syndrome Enzymatic deficiency FSH or LH receptor mutation |
24%–52% |
| Genital outflow tract and uterus | Congenital abnormality in M€ullerian development Congenital defect of urogenital sinus development |
15%–43% |
| Other | Thyroid disease Adrenal disease Complete androgen insensitivity Medications |
2%–8% |
| FSH = follicle-stimulating hormone; GnRH = gonadotropin-releasing hormone; LH = luteinizing hormone. | ||
EVALUATION OF THE PATIENT
Considerations in most patients with amenorrhea
History, physical examination, serum follicle-stimulating hormone (FSH) estimation, and estradiol (E2) will identify the most common causes of amenorrhea (Figs. 1 and 2). The presence of breast development means there has been previous estrogen action. Excessive testosterone secretion is suggested most often by hirsutism and rarely by increased muscle mass or other signs of virilization. The history and physical examination should include a thorough assessment of the external and internal genitalia as well as a breast examination. When the physical examination is normal (in most of the cases), the initial investigations should exclude pregnancy, estimate thyroid-stimulating hormone (TSH), and prolactin concentrations, and check FSH levels.
Thyroid disorders.
Both hypothyroidism and hyperthyroidism may result in chronic anovulation and amenorrhea. Even in the absence of thyroid-related symptoms, obtaining TSH in the setting of menstrual abnormalities is simple, inexpensive, and should be performed. Elevated TSH levels will be seen in primary hypothyroidism; conversely, TSH levels are suppressed in cases of hyperthyroidism, although levels may also be suppressed in secondary hypothyroidism and therefore clinical correlation is warranted when interpreting abnormal results. Abnormal TSH values should be followed up by a repeat value in addition to serum thyroxine (tetraiodothyronine; T4 or free T4) levels and treated accordingly. Estimation of TSH is useful to rule out subclinical hypothyroidism, even in the absence of thyroid-related symptoms, as treatment is warranted in the setting of menstrual irregularity or infertility (11).
Elevated prolactin levels.
Hyperprolactinemia may be associated with decreased E2 concentrations and amenorrhea or oligomenorrhea and is one of the more common causes of amenorrhea. However, only approximately 1/3 of women with hyperprolactinemia will have galactorrhea. Therefore, the absence of galactorrhea cannot reliably exclude women who may have amenorrhea from hyperprolactinemia (11). Prolactin concentrations are higher in women with amenorrhea than in those with oligomenorrhea (12), and it is, therefore, reasonable to check in all patients with these menstrual irregularities.
Prolactin levels <15–20 ng/mL in most clinical laboratories will exclude hyperprolactinemia. Circulating prolactin levels are fairly stable throughout the day but are transiently increased in numerous scenarios. Some of these include but are not limited to, sleeping, exercise, breast stimulation, a variety of drugs that lower dopamine levels or inhibit dopamine action, and eating. Prolactin levels that are mildly elevated (20–40 ng/mL) should be repeated and confirmed before the diagnosis of hyperprolactinemia is made. If they remain mildly elevated (and the patient is otherwise asymptomatic), a macroprolactin level should be considered. In addition, thyroid disorders should also be ruled out if prolactin is elevated. Elevated thyroid-releasing hormone can also cause stimulation of the pituitary lactotrophs, thus leading to pituitary hyperplasia and subsequent hyperprolactinemia (13–15).
Macroprolactin results from smaller prolactin molecules aggregating together that are bound by immunoglobulins, and has been reported to have a prevalence as high as nearly 20% of patients diagnosed with hyperprolactinemia (16). Macroprolactin is biologically inactive compared with the predominant circulating form of prolactin (80%–95%), called monomeric prolactin (17). Because of its low bioactivity, macroprolactinemia is often without any clinical symptoms such as galactorrhea.
Macroprolactinemia is confirmed by having the laboratory pretreat the patient’s serum with polyethylene glycol. This causes the macroprolactin to precipitate, thus separating the macroprolactin from the biologically active monomeric prolactin (18). Establishing this diagnosis avoids unnecessary and costly magnetic resonance imaging (MRI) imaging to evaluate for pituitary lesions (11).
Mildly elevated prolactin levels may be a sign of another organic central nervous system lesion, such as congenital aqueductal stenosis, nonfunctioning adenomas, or any condition that causes pituitary stalk inflammation. In women with hyperprolactinemia, the prevalence of a pituitary tumor is 50%–60% (8). The likelihood of a pituitary tumor is unrelated to the level of prolactin (19), and only 16% of the variability in tumor size is associated with prolactin level (r = 0.40, P<.001) (20). Therefore, an MRI should be performed whenever prolactin levels are persistently elevated. In most amenorrheic women with hyperprolactinemia, prolactin levels do not decline without treatment, and amenorrhea does not resolve as long as the prolactin levels remain elevated (12, 20). In the absence of another organic condition, dopamine agonists are the preferred treatment of hyperprolactinemia, with or without a pituitary tumor.
Figure 1
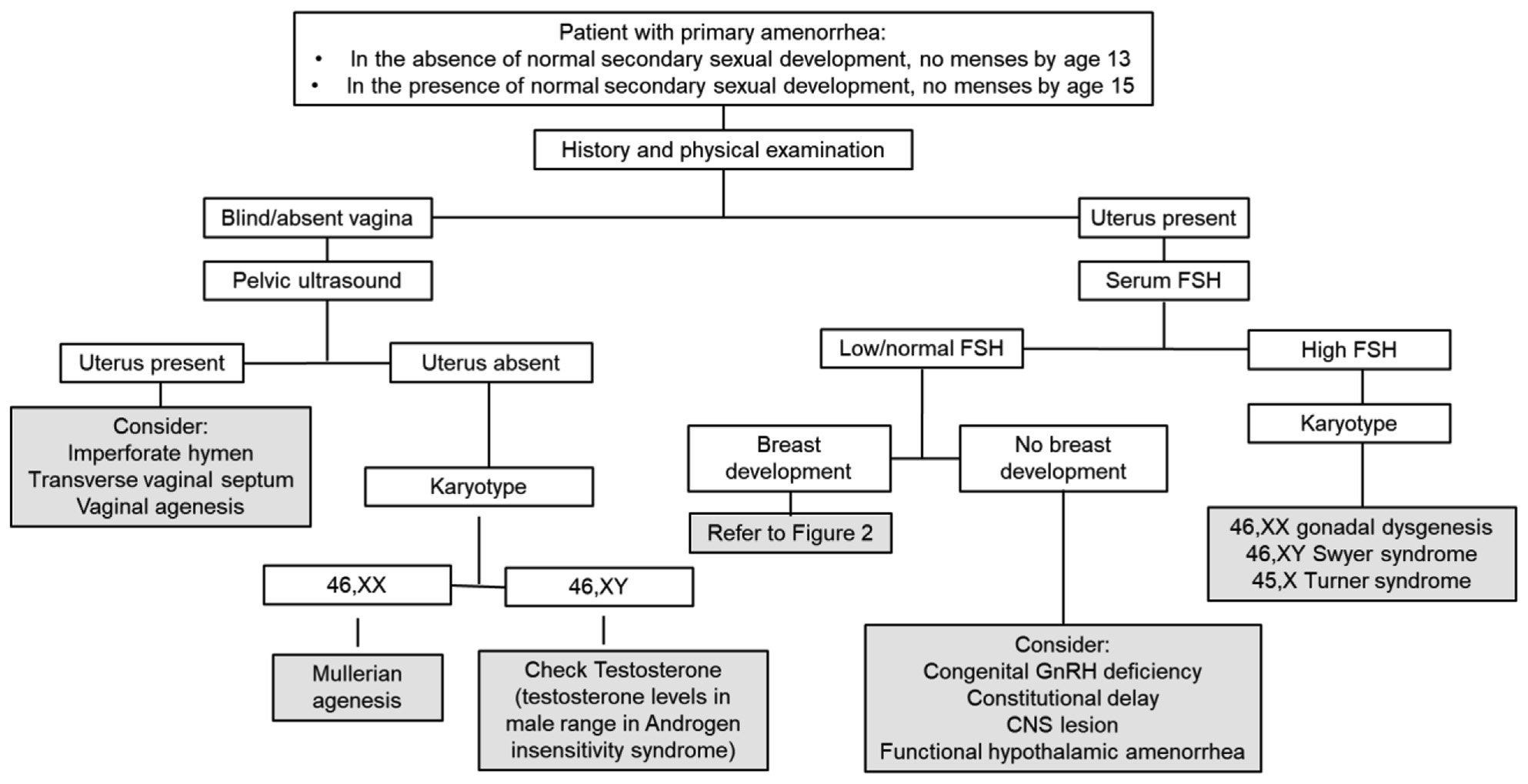
Figure 2
PRIMARY AMENORRHEA
Approach to evaluation
Physical examination.
Physical examination is key in evaluating primary amenorrhea (Fig. 1). In particular, a pelvic examination can provide important information, revealing abnormal findings in approximately 15% of patients with primary amenorrhea. A blind or absent vagina indicates outflow tract obstruction (as in imperforate hymen, transverse vaginal septum, or vaginal agenesis) or congenital absence of the uterus (as in M€ullerian agenesis or androgen insensitivity syndrome). Visualization of the cervix indicates the presence of a uterus. If a pelvic examination is not feasible, an abdominal ultrasound may be useful to confirm the presence or absence of the uterus. However, it is important to note that abdominal ultrasound may have limitations in its ability to detect a rudimentary or prepubertal uterus.
The presence of breast development indicates previous estrogen action. When breast development is absent, this finding is typically indicative of hypogonadism, including hypogonadotropic causes (congenital gonadotropinreleasing hormone [GnRH] deficiency, central nervous system lesions, functional hypothalamic amenorrhea [FHA]) and hypergonadotropic causes (gonadal dysgenesis and primary ovarian insufficiency [POI]).
Laboratory tests.
Depending on the findings elicited on physical examination, laboratory evaluation may be indicated. For example, if the congenital absence of the uterus is confirmed, karyotype and testosterone level are useful in distinguishing between M€ullerian agenesis and androgen insensitivity syndrome. In the case of a patient with a uterus but no breast development, measurement of serum FSH can differentiate between hypogonadotropic and hypergonadotropic causes. Many patients with primary amenorrhea will have evidence of both breast development and a uterus; in this case, laboratory evaluation similar to that which is conducted for secondary amenorrhea is appropriate (Fig. 2).
Specific causes.
Although most underlying causes of secondary amenorrhea can also present as primary amenorrhea, there are some conditions that present exclusively or more commonly as primary amenorrhea, and these diagnoses are covered in this section.
Anatomic defects
When all or part of the uterus and vagina are absent in the presence of otherwise normal female sexual characteristics, the diagnosis is usually M€ullerian agenesis, which accounts for approximately 15% of cases of primary amenorrhea. M€ullerian agenesis is often associated with urogenital malformations such as unilateral renal agenesis, pelvic kidney, horseshoe kidney, hydronephrosis, and ureteral duplication. M€ullerian agenesis must be differentiated from complete androgen insensitivity syndrome because the vagina may be absent or short in both disorders. Complete androgen insensitivity is rare, having an incidence as low as 1 in 60,000 (21), but it comprises approximately 5% of cases of primary amenorrhea (Table 1) (7, 22, 23). The simplest means of distinguishing between M€ullerian agenesis and complete androgen insensitivity is by measuring serum testosterone, which is in the normal male range or higher in the latter condition (24). Complete androgen insensitivity is suggested by family history, the absence of pubic hair, and the occasional presence of inguinal masses. The diagnosis can be confirmed by a 46, XY karyotype. The incidence of gonadal malignancy is 14%–22%, but it rarely occurs before the age of 20 (25, 26). Removal of the gonads should be offered through a patientcentered process after breast development and the attainment of adult stature. Individuals who undergo gonadectomy will require hormone replacement therapy.
Other anatomic defects include imperforate hymen (1 in 1,000 women), transverse vaginal septum (1 in 80,000 women), and isolated absence of the vagina or cervix (27). These conditions are more likely to present with complaints of cyclic pain and an accumulation of blood behind the obstruction rather than primary amenorrhea.
POI and Gonadal dysgenesis/agenesis
Lack of gonadal function is marked by high FSH levels. Gonadal failure can occur at any age, even in utero, when it is usually the result of gonadal agenesis or dysgenesis. Gonadal failure in genetically XX individuals is typically referred to as POI. When this occurs at any time before the onset of sexual maturation, there will be primary amenorrhea and incomplete breast development. Genetically XY individuals with gonadal failure will have female internal genitalia because antimϋllerian hormone (AMH) and testosterone will not be produced. Gonadal tumors occur in ≤25% of women with a Y chromosome. Unlike complete androgen insensitivity, these gonads do not secrete hormones and should be removed at the time of diagnosis (28).
Gonadal dysgenesis (streak gonads) can occur with normal XX and XY karyotypes and a variety of abnormal karyotypes, most commonly 45, X (Turner syndrome), in which oocyte loss is accelerated Add after 18 weeks in utero (29, 30). Turner syndrome is often diagnosed in early childhood because of the well-known phenotypic characteristics (short stature, webbed neck, and low hairline), and therefore, many patients do not present for assessment of primary amenorrhea. Uncommon causes of ovarian failure include FSH or luteinizing hormone (LH) receptor mutations (31, 32), galactosemia, 17 a-hydroxylase or 17,20-lyase deficiency, aromatase deficiency (33–35), and Blepharophimosis- Ptosis-Epicanthus inversus syndrome (FOXL2).
Hypogonadotropic hypogonadism
When hypogonadotropic hypogonadism is identified in an individual with primary amenorrhea, constitutional delay of puberty is a consideration but is a diagnosis of exclusion. Other potential etiologies include central nervous system lesions and FHA (both of which may explain cases of secondary amenorrhea, as well). One rare cause of hypogonadotropic hypogonadism is congenital gonadotropin deficiency. This is most often because of Kallmann syndrome, which is associated with defects in olfactory bulb development as a result of several different mutations. Thus, these women may have anosmia as well as amenorrhea and low gonadotropins because of GnRH deficiency (36). Mutations in GnRH receptor genes also may be associated with hypogonadotropic hypogonadism and may not have associated anosmia (37).
Table 2. Causes of secondary amenorrhea (7).
| Secondary amenorrhea | Approximate frequency | |
| Hypothalamus | Functional hypothalamic amenorrhea Inflammatory or infiltrative disease Infection Tumor Radiation Traumatic brain injury |
35% |
| Anterior pituitary | Hyperprolactinemia Pituitary tumors Pituitary infarction Space-occupying lesions Inflammatory and infiltrative disorders Radiation/surgery Infection |
17% |
| Ovary | Polycystic ovary syndrome Primary ovarian insufficiency Ovarian tumors Menopause |
40% |
| Genital outflow tract and uterus | Cervical stenosis Intrauterine synechiae |
7% |
| Other | Other chronic anovulation disorder Thyroid disease Adrenal disease Medications |
1% |
Table 3. Potential reasons for secondary amenorrhea.
| Class of medication |
|
SECONDARY AMENORRHEA
Approach to evaluation
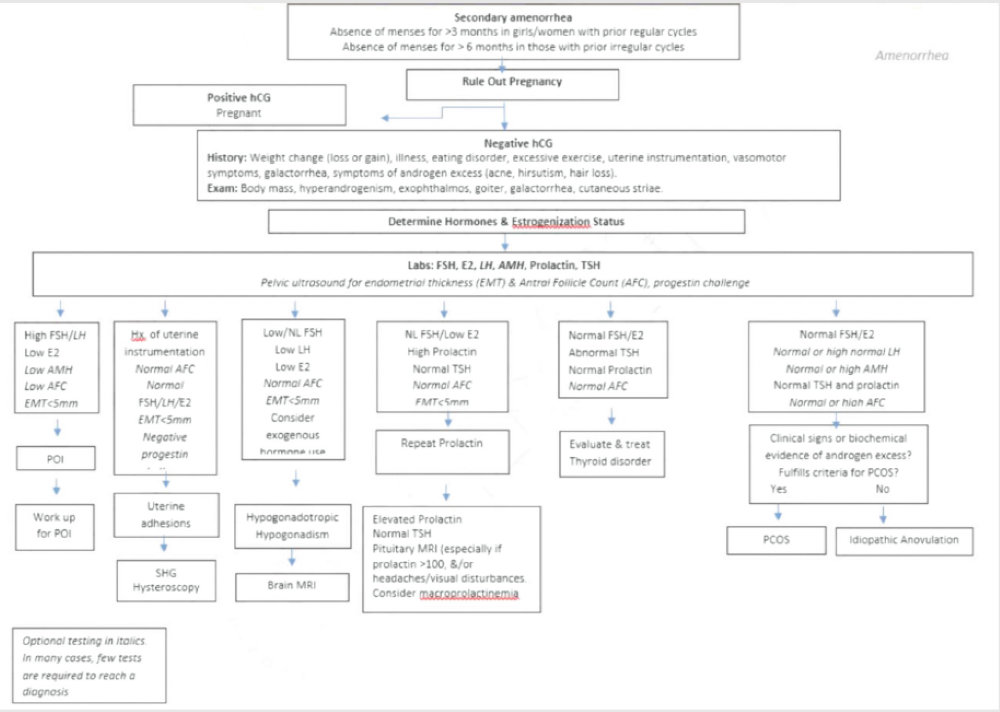
The possibility of pregnancy must be at the forefront of differential diagnoses for secondary amenorrhea. Once pregnancy has been ruled out, a stepwise approach to evaluation is recommended, as outlined in Figure 2. A thorough history is often illuminating. In contrast to primary amenorrhea, the diagnostic yield of physical examination alone is less for cases of secondary amenorrhea. Potential causes of secondary amenorrhea are listed in Table 2 (7). However, it should be noted that most surveys on the etiologies of secondary amenorrhea are dated, and with the expanded Rotterdam criteria for PCOS and increased prevalence of obesity, more patients may fall into the PCOS category today. A thorough history and reproductive hormone profile constitute the backbone of diagnostic evaluation, and pelvic ultrasound, if accessible and available, can help streamline evaluation early in the process. In many cases of secondary amenorrhea, only a few of the tests listed in Figure 2 are necessary to reach a diagnosis.
History.
The temporal pattern of menses since the onset of menarche is informative. For example, in cases of secondary amenorrhea developing against a backdrop of longstanding oligomenorrhea, conditions such as PCOS, disorders of the thyroid, disorders of the anterior pituitary (hyperprolactinemia, empty sella), hypothalamic-pituitary-ovarian (HPO) dysfunction associated with mental health disorders (depression, anxiety, and eating disorders) or consequent to iatrogenic influences (Table 3) and POI all merit consideration (38–48).
When new onset secondary amenorrhea develops in someone who previously had relatively predictable menses, beyond excluding pregnancy, disorders of mental and metabolic wellness (e.g., sudden and dramatic changes in body weight), as well as exogenous exposures, should be considered, when symptoms of hyperandrogenism are evident in the setting of secondary amenorrhea, PCOS is an obvious consideration. When the duration of symptoms and signs of hyperandrogenism is short (a few months) and the pace of symptomatic deterioration rapid (months), androgensecreting tumors (ovarian or adrenal) must be ruled out.
Anatomical causes for secondary amenorrhea must be considered when cessation of menses follows instrumentation of the uterine cavity (such as surgical termination of pregnancy, dilatation, and curettage for removal of retained productions of conception or retained placenta) or after hysteroscopic resection of submucous myoma, endometrial ablation, or pelvic vessel embolization (49, 50). History of an episode of postpartum hemorrhage predating the onset of secondary amenorrhea suggests Sheehan syndrome as a mechanism for secondary amenorrhea (51). Infectious etiology as a mechanism for endometrial scarring (such as genital tuberculosis) merits vigilance in select patient populations (52).
Physical examination.
The diagnostic yield of physical examination alone may be less for cases of secondary in comparison to primary amenorrhea. The presence of clinical hallmarks of goiter, thyroid bruit, and cutaneous and ocular signs can lead to a diagnosis of thyroid disorders, and in these cases, resumption of spontaneous menses is anticipated after the attainment of a euthyroid status. Features of hyperandrogenism (hirsutism, acne, and scalp hair thinning) suggest that PCOS-provided conditions such as late-onset congenital adrenal hyperplasia, hypothyroidism, and hyperprolactinemia are excluded. With evidence of virilization (worsening hirsutism, acne, bi-temporal recession of hair line, regression in breast size, deepening of voice, alterations in body fat and muscle mass, clitoromegaly, and increased libido), and in the absence of any suspicion for exposure to exogenous androgens, androgen-secreting tumor of the ovary or adrenal gland must be excluded. If blood pressure readings are elevated, specific clinical stigmata of purple striae along the abdominal wall and accumulation of dorsal cervical fat pad should be looked for, and Cushing syndrome or disease be considered in the differential diagnosis (53). Subjective complaints or objective evidence of galactorrhea would point toward hyperprolactinemia as a mechanism for secondary amenorrhea (54). Evidence of central adiposity and acanthosis nigricans should prompt consideration for insulin resistance as a mechanism for PCOS-like phenotype and for HPO dysfunction.
Laboratory tests
Pregnancy test.Pregnancy as a mechanism for secondary amenorrhea must be the first consideration. False negative urinary pregnancy test readings are plausible, and hence, checking blood levels of human chorionic gonadotropin may be preferred in appropriate clinical settings.
FSH, LH, and E2 levels.Once pregnancy as a mechanism for secondary amenorrhea has been ruled out, random measurement of levels of the pituitary gonadotropins along with E2 (the major circulating estrogen in reproductive-age women that is predominantly of ovarian origin) will differentiate between secondary amenorrhea resulting from an exhaustion of the ovarian reserve (such as POI, when the picture will be that of hypergonadotropic hypogonadism) from all other causes of secondary amenorrhea. In normo-ovulatory women, serum levels of E2 fluctuate between low but detectable levels in the early follicular phase (often in the range of 30–50 pg/ mL) to peak preovulatory levels (range of 150–300 pg/mL). This contrasts with FHA, where circulating E2 is more in the menopausal range (<30 pg/mL), whereas levels of gonadotropins are in the normal to low normal range; LH levels are often disproportionately lower than FSH in cases of FHA. In contrast, disproportionately elevated LH levels in relation to FSH are not uncommonly encountered in women with PCOS.
Ovarian reserve markers.AMH is produced by granulosa cells of pre-antral and antral stage ovarian follicles and is a reliable reflection of the ovarian reserve. Disproportionately elevated levels of AMH are commonly encountered in cases of PCOS (particularly when polycystic ovarian morphology is one of the diagnostic criteria); levels are tightly correlated with the ovarian antral follicle count. Conversely, undetectable levels of AMH are consistent with decreased ovarian reserve (55) and are observed in women with POI. Although ovarian reserve markers such as AMH may be useful in the diagnosis of some causes of amenorrhea, they are frequently not necessary and should be interpreted with caution (ASRM PC).
Prolactin.As previously described, hyperprolactinemia is a recognized mechanism for secondary amenorrhea, and hence checking prolactin levels must be included in the initial workup of not just of secondary amenorrhea but also in evaluating disorders of menstrual regularity (56). Circulating levels in the range of 15–20 ng/mL will exclude hyperprolactinemia as a cause of amenorrhea. In the workup of hyperprolactinemia, macroprolactinemia (molecular weight >100 kDa) must be considered as a mechanism for persistently elevated prolactin levels (57). Establishing this diagnosis avoids unnecessary and costly MRI imaging to evaluate for pituitary lesions (7). However, unlike the predominant monomeric form of circulating prolactin, macroprolactin is biologically inert, and hence, macroprolactinemia is unlikely to be a cause of secondary amenorrhea.
Thyroid function tests.TSH is considered among the firstline screening tests in any reproductive-age woman presenting with menstrual abnormalities including secondary amenorrhea. Although considered the gold standard for evaluation of thyroid function, it is important to appreciate that interpretability is limited when dealing with secondary hypothyroidism because of pituitary insufficiency, as seen in Sheehan’s syndrome; in the latter situation, free thyroxine levels should additionally be tested. In addition, mild thyroid function abnormalities, such as subclinical hypothyroidism, can co-exist with other pathologies. Therefore, the identification of these diagnoses should not preclude consideration of other etiologies of amenorrhea.
Androgens and androgen precursors.Testing should be consideredwhen features of hyperandrogenismaccompany secondary amenorrhea. Serum levels of testosterone (total and free) and dehydroepiandrosterone sulfate (DHEAS) allow insights into the source of androgen overproduction (ovarian and adrenal, respectively). Screening for 21 hydroxylase deficiency (the commonest form of late-onset congenital adrenal hyperplasia) is based on serum levels of 17 hydroxyprogesterone.
Radiological tests
Pituitary imaging.Persistently elevated prolactin levels merit further investigation with pituitary imaging (MRI being the preferred modality) to examine for a central mechanism for hyperprolactinemia as a pituitary adenoma may be identified in 50%–60% of cases of persistent hyperprolactinemia (18). The likelihood of a pituitary tumor is unrelated to the level of prolactin excess. Although a functioning pituitary adenoma is the most common of structural causes for hyperprolactinemia, uncommonly, conditions such as pseudotumor cerebri, empty sella, congenital aqueductal stenosis, and nonfunctioning adenomas can also cause mild elevations in prolactin levels.
Pelvic ultrasound.Preferably undertaken via transvaginal route if feasible, pelvic ultrasound can be highly informative and, if accessible and available, should be considered at the forefront of investigations for the evaluation of secondary amenorrhea (Fig. 2). Ultrasound measures of endometrial thickness and trilaminar endometrial echo pattern correlate well with the estrogenic milieu (19). Aspects of ovarian morphology (ovarian volume, number, and distribution pattern of antral follicles) offer reliable assessment of ovarian reserve and contribute validated criteria (on the basis of antral follicle count and ovarian volume indices) for allowing a diagnosis of PCOS, whereas abnormalities such as complex ovarian masses with abnormal vascular flow can guide expeditious evaluation for hormone secreting ovarian tumor as a mechanism for secondary amenorrhea.
Inappropriate historical settings, an attenuated hyperechoic endometrial echo can raise suspicion for endometrial scarring; this impression must prompt further investigation either by saline infusion sonography or diagnostic hysteroscopy.
Miscellaneous tests
Screening tests for mycobacterium tuberculosis.(PPD or serum Quantiferon-Gold) should be considered in appropriate clinical settings. Endometrial sampling for evaluation (by histological evaluation and/or PCR for mycobacterium TB) of tuberculous endometritis merits consideration in high-risk patient populations. Diagnostic hysteroscopy remains the gold standard methodology for evaluating the endometrial cavity.
Anterior pituitary hormones.In addition to the pituitary gonadotropins and prolactin mentioned earlier, testing of other hormones secreted by the anterior pituitary (adrenocorticotropin and growth hormone) should be considered in appropriate clinical settings, such as in the evaluation of Sheehan’s syndrome. Growth hormone excess may present as normo-prolactinemic galactorrhea (4, 58).
Dynamic test.The progesterone withdrawal test (PWT) or progesterone challenge test (PCT) (59): the foundation of this test centers on the understanding that although low E2 and high gonadotropin levels are informative of ovarian insufficiency, normal E2 levels (in the range that is deemed normal for early follicular phase) and normal gonadotropins are relatively poor discriminants of the many nonovarian causes of amenorrhea. The premise of PWT lies in the provocation of tissue death and shedding of estrogenized endometrium after transient exposure to and then withdrawal of progesterone or progestin ‘‘challenge.’’ In amenorrheic women, evidence of bleeding (regardless of amount) after a course of progestin or progesterone is consistent with a picture of anovulation as a mechanism for amenorrhea. Interpretation of a failed response (i.e., no bleeding) to PWT can be twofold: secondary to a hypoestrogenic milieu, as seen in the state of menopause or FHA and because of an inability of the endometrium to respond to an estrogen replete environment (as seen in cases of Asherman syndrome). Histological evidence of endometrial proliferation is evident even with circulating E2 levels in the early follicular phase (levels that are commonly seen in anovulatory women with PCOS). This contrasts with FHA, where circulating E2 is suppressed (<30 pg/mL), and the endometrium is often quiescent. In amenorrheic women, ultrasound findings of endometrial thickness can help guide decisions regarding proceeding with PWT. The absence of withdrawal bleeding with a progestin challenge is predictable, if ultrasound demonstrates an attenuated endometrium. In this setting, a combination of estrogen plus progestin may be a better strategy to differentiate between amenorrhea because of hypoestrogenemia and that resulting from endometrial scarring (Fig. 2). Because both false positive and negative PWT can occur, clinical correlation is indicated in the interpretation of test results (60, 61). Although the PWT may still have a role in the evaluation of amenorrhea, other described approaches may result in a more rapid and accurate diagnosis.
CONCLUSIONS
- Most of the causes of primary and secondary amenorrhea are similar.
- Most cases of amenorrhea are accounted for by six conditions: polycystic ovary syndrome, thyroid disorders, hyperprolactinemia, hypogonadotropic and hypergonadotropic hypogonadism, and anatomic abnormalities once congenital abnormalities are ruled out.
- History, physical examination, and estimation of serum FSH and estradiol will identify the most common causes of amenorrhea.
- Most patients presenting with amenorrhea should undergo measurements of serum prolactin and TSH, and pregnancy should be excluded.
- Physical examination and measurement of gonadotropins are key in the evaluation of primary amenorrhea.
- The diagnostic yield of physical examination alone may be less for cases of secondary in comparison to primary amenorrhea.
Acknowledgments
This report was developed under the direction of the Practice Committee of the American Society for Reproductive Medicine as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or to dictate an exclusive course of treatment. Other plans of management may be appropriate, taking into account the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice Committee and the Board of Directors of the American Society for Reproductive Medicine have approved this report. This document was reviewed by ASRM members, and their input was considered in the preparation of the final document. The following members of the ASRM Practice Committee participated in the development of this document: Alan Penzias, M.D.; Paula Amato, M.D.; Jacob Anderson, M.B.A.; Kristin Bendikson, M.D.; Clarisa Gracia, M.D., M.S.C.E.; Tommaso Falcone, M.D.; Rebecca Flyckt, M.D.; Jessica Goldstein, R.N.; Karl Hansen, M.D., Ph.D.; Micah Hill, D.O.; Sangita Jindal, Ph.D.; Suleena Kalra, M.D., M.S.C.E.; Tarun Jain, M.D.; Bruce Pier, M.D.; Michael Thomas, M.D.; Richard Reindollar, M.D.; Jared Robins, M.D.; Chevis N. Shannon, Dr.Ph., M.B.A., M.P.H.; Anne Steiner, M.D., M.P.H.; Cigdem Tanrikut, M.D.; and Belinda Yauger, M.D. The Practice Committee acknowledges the special contribution of Karl Hansen, M.D., Ph.D.; Blake Evans, D.O.; Jacqueline Lee, M.D.; Shelby Neal, M.D.; and Lubna Pal, M.D. in the preparation of this document. All Committee members disclosed commercial and financial relationships with manufacturers or distributors of goods or services used to treat patients. Members of the Committee who were found to have conflicts of interest on the basis of the relationships disclosed did not participate in the discussion or development of this document.
REFERENCES
- Stedman’s Medical Dictionary. 27th ed. Philadelphia: Lippincott Williams & Wilkins; 2000:56.
- Herman-Giddens ME, Slora EJ, Wasserman RC, Bourdony CJ, Bhapkar MV, Koch GG, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99:505–12.
- Pettersson F, Fries H, Nillius SJ. Epidemiology of secondary amenorrhea. I. Incidence and prevalence rates. Am J Obstet Gynecol 1973;117:80–6.
- Bachmann GA, Kemmann E. Prevalence of oligomenorrhea and amenorrhea in a college population. Am J Obstet Gynecol 1982;144:98–102.
- Taylor HS, Pal L, Seli E. Amenorrhea. In: Speroff's clinical gynecologic endocrinology and infertility. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2020:343–94.
- Reindollar RH, Byrd JR, McDonough PG. Delayed sexual development: a study of 252 patients. Am J Obstet Gynecol 1981;140:371–80.
- Reindollar RH, Novak M, Tho SP, McDonough PG. Adult-onset amenorrhea: a study of 262 patients. Am J Obstet Gynecol 1986;155:531–43.
- Kwon SK, Chae HD, Lee KH, Kim SH, Kim CH, Kang BM. Causes of amenorrhea in Korea: experience of a single large center. Clin Exp Reprod Med 2014;41:29–32.
- Diaz A, Lipman Diaz EG. Disorders of sex development. Pediatr Rev 2021;42: 414–26.
- Witchel SF. Congenital adrenal hyperplasia. J Pediatr Adolesc Gynecol 2017; 30:520–34.
- Taylor HS, Pal L, Seli E. Amenorrhea. In: Speroff's clinical gynecologic endocrinology and infertility. Philadelphia: Lippincott Williams & Wilkins; 2020: 1036.
- Touraine P, Plu-Bureau G, Beji C, Mauvais-Jarvis P, Kuttenn F. Long-term follow-up of 246 hyperprolactinemic patients. Acta Obstet Gynecol Scand 2001;80:162–8.
- Danziger J, Wallace S, Handel S, Samaan NB. The sella turcica in primary end organ failure. Radiology 1979;131:111–5.
- Sarlis NJ, Brucker-Davis F, Doppman JL, Skarulis MC. MRI-demonstrable regression of a pituitary mass in a case of primary hypothyroidism after a week of acute thyroid hormone therapy. J Clin Endocrinol Metab 1997; 82:808–11.
- Kanasaki H, Oride A, Mijiddorj T, Kyo S. Role of thyrotropin-releasing hormone in prolactin-producing cell models. Neuropeptides 2015;54:73–7.
- Kalsi AK, Halder A, Jain M, Chaturvedi PK, Sharma JB. Prevalence and reproductive manifestations of macroprolactinemia. Endocrine 2019;63:332–40.
- Hattori N, Inagaki C. Anti-prolactin (PRL) autoantibodies cause asymptomatic hyperprolactinemia: bioassay and clearance studies of PRLimmunoglobulin G complex. J Clin Endocrinol Metab 1997;82:3107–10.
- Gibney J, Smith TP, McKenna TJ. Clinical relevance of macroprolactin. Clin Endocrinol (Oxf) 2005;62:633–43.
- Brenner SH, Lessing JB, Quagliarello J, Weiss G. Hyperprolactinemia and associated pituitary prolactinomas. Obstet Gynecol 1985;65:661–4.
- Schlechte J, Dolan K, Sherman B, Chapler F, Luciano A. The natural history of untreated hyperprolactinemia: a prospective analysis. J Clin Endocrinol Metab 1989;68:412–8.
- Jagiello G. Prevalence of testicular feminization. Lancet 1962;1:329.
- Rarick LD, Shangold MM, Ahmed SW. Cervical mucus and serum estradiol as predictors of response to progestin challenge. Fertil Steril 1990;54:353–5.
- Tanmahasamut P, Rattanachaiyanont M, Dangrat C, Indhavivadhana S, Angsuwattana S, Techatraisak K. Causes of primary amenorrhea: a report of 295 cases in Thailand. J Obstet Gynaecol Res 2012;38:297–301.
- Wilson JD. Syndromes of androgen resistance. Biol Reprod 1992;46:168– 73.
- Lobo RA. Primary and secondary amenorrhea. In: Fraser IS, Jansen R, Lobo RA, Whitehead M, editors. Estrogens and progestogens in clinical practice. London: Churchill Livingstone; 1998.
- Deans R, Creighton SM, Liao L-M, Conway GS. Timing of gonadectomy in adult women with complete androgen insensitivity syndrome (CAIS): patient preferences and clinical evidence. Clin Endocrinol (Oxf) 2012;76:894–8.
- Reid RL. Amenorrhea. In: Copeland LJ, editor. Textbook of gynecology. 2nd ed. Philadelphia: WB Saunders; 1996.
- Manuel M, Katayama PK, Jones HW Jr. The age of occurrence of gonadal tumors in intersex patients with a Y chromosome. Am J Obstet Gynecol 1976;124:293–300.
- Turner HH. A syndrome of infantilism, congenital webbed neck, and cubitus valgus. Endocrinology 1938;23:566–74.
- Turner’s syndrome. West J Med 1982;137:32–44.
- Toledo SP, Brunner HG, Kraaij R, Post M, Dahia PL, Hayashida CY, et al. An inactivating mutation of the luteinizing hormone receptor causes amenorrhea in a 46,XX female. J Clin Endocrinol Metab 1996;81:3850–4.
- Aittomaki K, Lucena JL, Pakarinen P, Sistonen P, Tapanainen J, Gromoll J, et al. Mutation in the follicle-stimulating hormone receptor gene causes hereditary hypergonadotropic ovarian failure. Cell 1995;82:959–68.
- Allingham-Hawkins DJ, Babul-Hirji R, Chitayat D, Holden JJ, Yang KT, Lee C, et al. Fragile X premutation is a significant risk factor for premature ovarian failure: the International Collaborative POF in fragile X study—preliminary data. Am J Med Genet 1999;83:322–5.
- Laml T, Preyer O, Umek W, Hengstschlager M, Hanzal H. Genetic disorders in premature ovarian failure. Hum Reprod Update 2002;8:483–91.
- Morishima A, Grumbach MM, Simpson ER, Fisher C, Qin K. Aromatase deficiency in male and female siblings caused by a novel mutation and the physiological role of estrogens. J Clin Endocrinol Metab 1995;80:3689–98.
- Hall JE. Physiologic and genetic insights into the pathophysiology and management of hypogonadotropic hypogonadism. Ann Endocrinol 1999;60: 93–101.
- Layman LC, McDonough PG, Cohen DP, Maddox M, Tho SP, Reindollar RH. Familial gonadotropin-releasing hormone resistance and hypogonadotropic hypogonadism in a family with multiple affected individuals. Fertil Steril 2001;75:1148–55.
- Klein DA, Paradise SL, Reeder RM. Amenorrhea: a systematic approach to diagnosis and management. Am Fam Phys 2019;100:39–48.
- Warren MP, Fried JL. Hypothalamic amenorrhea. The effects of environmental stresses on the reproductive system: a central effect of the central nervous system. Endocrinol Metab Clin North Am 2001; 30:611–29.
- Azziz R. Reproductive endocrinologic alterations in female asymptomatic obesity. Fertil Steril 1989;52:703–25.
- Pandey S, Bhattacharya S. Impact of obesity on gynecology. Womens Health (Lond) 2010;6:107–17.
- Glass AR, Dahms WT, Abraham G, Atkinson RL, Bray GA, Swerdloff RS. Secondary amenorrhea in obesity: etiologic role of weight-related androgen excess. Fertil Steril 1978;30:243–4.
- Fourman LT, Fazeli PK. Neuroendocrine causes of amenorrhea-an update. J Clin Endocrinol Metab 2015;100:812–24.
- Lambrinoudaki I, Paschou SA, Lumsden MA, Faubion S, Makrakis E, Kalantaridou S, et al. Premature ovarian insufficiency: a toolkit for the primary care physician. Climacteric 2021;24:425–37.
- Welt CK. Primary ovarian insufficiency: a more accurate term for premature ovarian failure. Clin Endocrinol (Oxf) 2008;68:499–509.
- Fonseca BM, Rebelo I. Cannabis and cannabinoids in reproduction and fertility: where we stand. Reprod Sci 2022;29:2429–39.
- Mello NK, Mendelson JH, Kelly M, Diaz-Migoyo N, Sholar JW. The effects of chronic cocaine self-administration on the menstrual cycle in rhesus monkeys. J Pharmacol Exp Ther 1997;281:70–83.
- Mello NK,Mendelson JH. Cocaine's effects on neuroendocrine systems: clinical and preclinical studies. Pharmacol Biochem Behav 1997;57:571–99.
- March CM. Asherman’s syndrome. Semin Reprod Med 2011;29:83–94.
- Davies C, Gibson M, Holt EM, Torrie EP. Amenorrhoea secondary to endometrial ablation and Asherman's syndrome following uterine artery embolization. Clin Radiol 2002;57:317–8.
- Kele¸stimur F. Sheehan's syndrome. Pituitary 2003;6:181–8.
- Fowler ML, Mahalingaiah S. Case report of pelvic tuberculosis resulting in Asherman’s syndrome and infertility. Fertil Res Pract 2019;5:8.
- Morton A. A devastating cause of amenorrhoea. J Obstet Gynaecol 2013; 33:532–4.
- Glezer A, Bronstein MD. Hyperprolactinemia. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dhatariya K, et al., editors. Endotext [Internet]. South Dartmouth, MA: MDText.com, Inc.; 2000.
- Tehrani FR, Firouzi F, Behboudi-Gandevani S. Investigating the clinical utility of the anti-Mullerian hormone testing for the prediction of age at menopause and assessment of functional ovarian reserve: a practical approach and recent updates. Aging Dis 2022;13:458–67.
- Practice Committee of the American Society for Reproductive Medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril 2020;114:1151–7.
- Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med 2002;20:365–74.
- Fleischer AC, Kalemeris GC, Entman SS. Sonographic depiction of the endometrium during normal cycles. Ultrasound Med Biol 1986;12:271–7.
- Goldman MH, Klinges K. Acromegaly as the amenorrhea-galactorrhea syndrome. N J Med 1989;86:887–8.
- Progestogen challenge test––Wikipedia. Available at: https://en.wikipedia. org/wiki/Progestogen_challenge_test. Accessed January 20, 2023.
- Nakamura S, Douchi T, Oki T, Ijuin H, Yamamoto S, Nagata Y. Relationship between sonographic endometrial thickness and progestin-induced withdrawal bleeding. Obstet Gynecol 1996;87:722.
Practice Documents
ASRM Practice Documents have been developed to assist physicians with clinical decisions regarding the care of their patients.
Artificial intelligence in the in vitro fertilization laboratory: a committee opinion (2026)
Artificial intelligence has already been portrayed as a tool that will impact different areas of laboratory function, most importantly embryo selection.
Fertility care and family building for LGBTQ+ individuals: a committee opinion (2026)
The purpose of this ASRM Practice Committee Opinion is to provide clinicians with strategies and special considerations for the evaluation and treatment of individuals in the LGBTQ+ community.
Intracytoplasmic sperm injection for nonmale factor indications: a Committee opinion (2026)
ICSI use extends beyond male infertility, raising questions about benefits when semen parameters meet WHO reference values.
The International Glossary on Infertility and Fertility Care, 2025
Previous editions of the International Glossary on Infertility and Fertility Care established internationally recognized definitions related to clinical practice, research, and policy.More Resources
ASRM Practice Documents

ASRM MAC Tool 2021
The ASRM Müllerian Anomaly Classification 2021 (MAC2021) includes cervical and vaginal anomalies and standardize terminology within an interactive tool format.

Coding Corner Q & A
The Coding Corner Q & A is a list of previously submitted and answered questions from ASRM members about coding. Answers are available to ASRM Members only.

EMR Shared Phrases/Template Library
This resource includes phrases shared by ASRM physician members to provide a template for individuals to create their own EMR phrases.

ASRM Ethics Opinions
Ethics Committee Reports are drafted by the members of the ASRM Ethics Committee on the tough ethical dilemmas of reproductive medicine.

COVID-19 Resources
A compendium of ASRM resources concerning the Novel Corona virus (SARS-COV-2) and COVID-19.

Patient Resources
ReproductiveFacts.org provides a wide range of information related to reproductive health and infertility through patient education fact sheets, infographics, videos, and other resources.