

Evidence-based diagnosis and treatment for uterine septum: a guideline
Download a PDF of this documentMethods: This guideline provides evidence-based recommendations regarding the diagnosis and effectiveness of surgical treatment of a uterine septum. This replaces the last version of the same name (Fertil Steril. 2016 Sep 1;106(3):530-40).
Main Outcome Measure(s): Outcomes of interest included the impact of a septum on underlying fertility, live birth, clinical pregnancy, and obstetrical outcomes.
Result(s): The literature search identified relevant studies to inform the evidence for this guideline.
Conclusion(s): The treatment of uterine septa and subsequent outcomes associated with infertility, recurrent pregnancy loss, and adverse obstetrical outcomes are summarized. Resection of a septum has been shown to improve outcomes in patients with recurrent pregnancy loss and to decrease the likelihood of malpresentation. In the setting of infertility, it is recommended to use a shared decision-making model after appropriate counseling to determine whether or not to proceed with septum resection. (Fertil Steril® 2024;122: 251–65. ©2024 by American Society for Reproductive Medicine.)
RECOMMENDATIONS
- It is recommended to use 3D transvaginal ultrasound with or without saline infusion as the first-line noninvasive diagnostic tool in uterine shape assessment. (Strength of Evidence: B; Strength of Recommendation: Moderate).
- No recommendation can be made regarding the association between a septate uterus and infertility due to insufficient evidence. (Strength of Evidence: C; Strength of recommendation: No recommendation).
- It is recommended to counsel patients that the presence of a septate uterus is associated with spontaneous abortion and obstetric complications. (Strength of Evidence: B; Strength of Recommendation: Moderate).
- Although septum incision in patients with infertility and/or undergoing fertility treatment is reasonable, a firm recommendation for this practice cannot be made on the basis of the current evidence. It is recommended to counsel patients with infertility and/or undergoing fertility treatment that resection of septum may or may not be associated with an increase in live births. Given limitations in the literature and the low risk of the procedure, septum incision may be offered to patients in a shared decision-making model. (Strength of Evidence: B; Strength of Recommendation: Moderate).
- It is recommended to offer hysteroscopic septum incision to patients with a septum and a history of recurrent miscarriage in a shared decision-making model. (Strength of Evidence: B; Strength of Recommendation: Moderate).
- It is recommended to counsel patients that septum incision may decrease the risk of adverse obstetric outcomes such as malpresentation and cesarean section, but there are no high-quality data to recommend this practice. (Strength of Evidence:B; Strength of Recommendation:Moderate).
- It is not recommended to use septum characteristics such as size or shape to determine the impact on adverse reproductive outcomes. (Strength of Evidence: B/C; Strength of recommendation: Moderate/Weak).
- It is recommended, on the basis of expert committee opinion, to consider performing the procedure during the follicular phase or after progesterone withdrawal to help with visualization during surgery. However, there are no studies designed to prove or disprove this. (Strength of Evidence: Insufficient; Strength of recommendation: Weak).
- It is recommended to counsel patients that, on the basis of limited data, there is no evidence that resection of the unicollis cervical septum increases the risk of cervical insufficiency. (Strength of Evidence: C; Strength of recommendation: Weak).
- It is not recommended to perform another surgery for a residual septum under 1 cm. (Strength of Evidence: C; Strength of recommendation: Weak).
- There is insufficient evidence to recommend routine administration of oral estrogen, intrauterine balloons, and IUDs to decrease adhesion formation after resection of a septum. (Strength of Evidence: C; Strength of recommendation: Weak).
- It appears the rate of uterine rupture after resection of a septum is rare; however, this outcome is not often reported on in the current literature. (Strength of Evidence: B/C; Strength of recommendation: Moderate/Weak).
- It is recommended to counsel patients that they may proceed with fertility treatment in 1-2 months after resection of a septum. (Strength of Evidence: C; Strength of recommendation: Weak).
- There is insufficient evidence to recommend hysteroscopic resection of a septum in patients who have not yet attempted conception (Strength of Evidence: Insufficient Strength of recommendation: Insufficient evidence to make recommendation).
Müllerian anomalies are rare developmental anomalies of the reproductive tract. These anomalies are typically viewed as defects of fusion of the Müllerian (paramesonephric) ducts or canalization failures after fusion or both. A uterine septum occurs when the tissue connecting the 2 paramesonephric ducts fails to resorb before the 20th embryonic week. The presence of a uterine septum has been associated with infertility, recurrent miscarriage, and poor obstetrical outcomes such as preterm birth (1). The true prevalence of uterine septa is difficult to ascertain as uterine septa are often asymptomatic but appear to range between 1 and 2 per 1,000 to as frequent as 15 per 1,000 (2).
Initially, uterine septa were believed to be predominantly fibrous tissue covered by endometrium. However, biopsy specimens and magnetic resonance imaging (MRI) imaging suggest that septa are composed primarily of muscle fibers and less connective tissue (3–5).
Müllerian duct anomalies, such as unicornuate uterus and uterine didelphys, are associated with concurrent renal anomalies in approximately 11%–30% of individuals (6). However, data do not suggest an association between the septate uterus and renal anomalies, and, as such, it is not necessary to routinely evaluate the renal system in patients with a uterine septum.
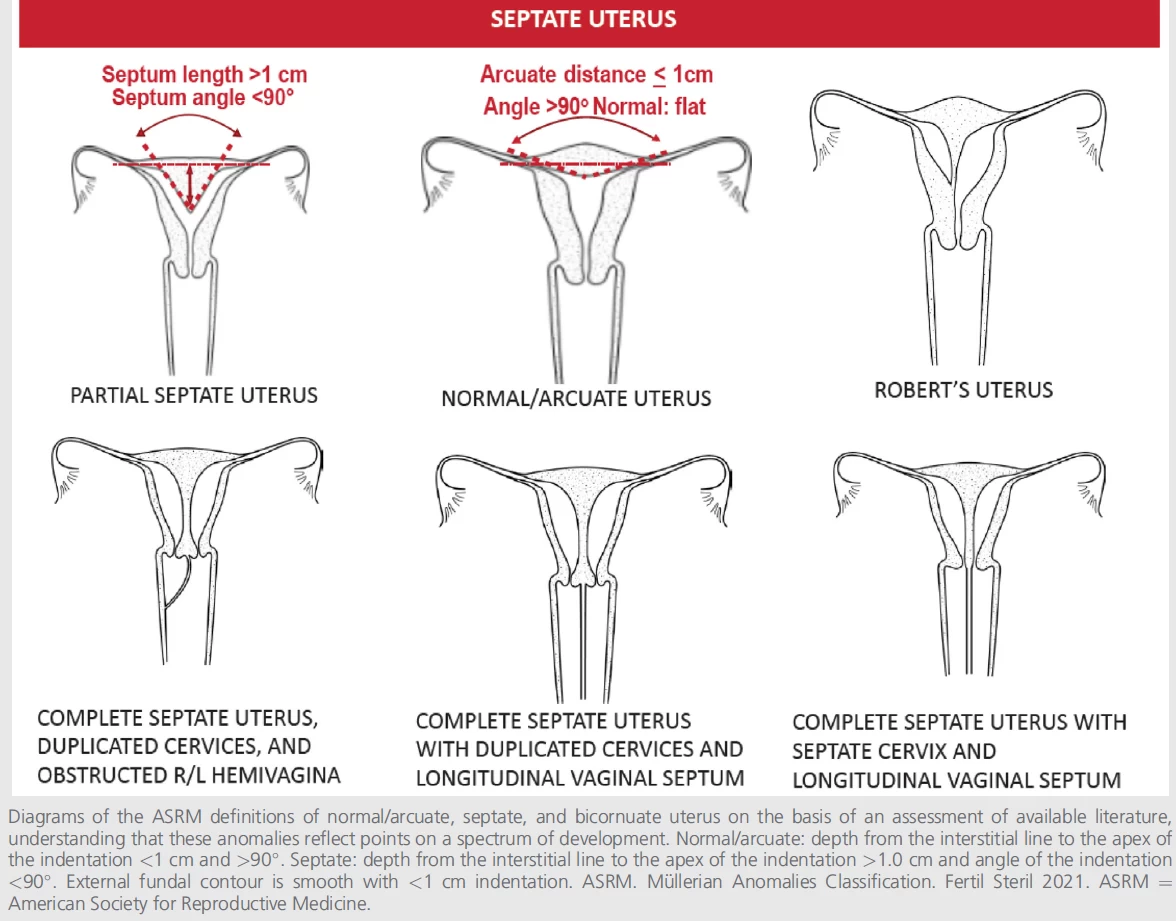
Septate uteri have a spectrum of configurations ranging from an incomplete/partial septate to a complete septate uterus. A partial septate uterus refers to a single fundus and cervix with a uterine septum extending from the top of the endometrial cavity toward the cervix. The size and shape of the septum can vary by width, length, and vascularity. Although developmentally, the arcuate uterus may be considered as part of the spectrum of Müllerian anomalies, it is typically considered a normal variant and therefore functionally not part of the septate spectrum. The original American Fertility Society (AFS) classification system placed the arcuate uterus in its own category as, in contrast to other uterine malformations, it is not associated with adverse clinical outcomes (7). However, it is important to differentiate arcuate from septate uterus to better direct surgical intervention, when appropriate, for the septate uterus. In the revised American Society for Reproductive Medicine (ASRM) classification (Fig. 1), the arcuate uterus configuration is placed in the septate uterus box with a clear description.
CLASSIFICATION
There are many proposed classification systems for Müllerian anomalies. The AFS classification from 1988 has been the most recognized and used (7). Many other classification systems have been developed to address limitations of the AFS classification such as exclusion of anomalies of the vagina and cervix, lack of clear diagnostic criteria, and inability to classify complex aberrations. The ASRM Task Force on Müllerian Anomalies Classification was formed and charged with designing a new classification to address the identified limitations. The Task Force set goals for a new classification and chose to base it on the iconic AFS classification from 1988 because of its simplicity and recognizability while expanding and updating it to include all categories of anomalies. The pictorial representation of this classification was published and shown in Figure 1. Literature searches were performed using all terms pertaining to uterine septum. The uterine septum may be associated with vaginal anomalies such as a longitudinal vaginal septum or obstructed hemivagina. This document will not cover the management of the vaginal anomalies. The management of cervical anomalies such as duplicated or septate cervix will be discussed.LIMITATIONS OF THE LITERATURE
Multiple challenges exist in interpreting the literature related to the effectiveness and safety of the management of a uterine septum. Most studies compare outcomes pre and postsurgery without comparison with an untreated control group, which is problematic given the significant rate of unassisted pregnancy with expectant management. Moreover, many studies are underpowered, and some report only surrogate outcomes such as clinical or ongoing pregnancy rather than live birth. In addition, the numerous and varied definitions and terminology used to describe the septate uterus make it challenging to interpret the data. Variable durations of infertility or the number of pregnancy losses before surgical intervention also makes comparisons between studies difficult, given the strong correlation between infertility and recurrent pregnancy loss duration and treatment outcomes. In addition, variations in surgical technique, experience, and approach are not well accounted for in the existing literature.Figure 1
METHODS
This clinical practice guideline followed a methodological protocol established by ASRM staff and executive leadership, the ASRM Practice Committee, and an independent consulting epidemiologist. The ASRM Practice Committee identified the necessity to update the previously published guideline on uterine septum and empaneled a task force of experts to engage in its development. Members of the task force applied the Population, Interventions, Comparisons, and Outcomes framework to formulate focused questions related to clinical practice and evidence-based treatments for uterine septum, as well as preliminary inclusion/exclusion criteria.This guideline provides evidence-based recommendations for surgical treatment in different clinical scenarios, such as infertility and recurrent pregnancy loss.
A comprehensive systematic review of the literature using the MEDLINE® database through PubMed® was conducted to identify peer-reviewed studies relevant to treatments for uterine septum. This document is an update to the previously published uterine septum guideline (2016). The searches were restricted to include papers published since the previous guideline with a date range of April 1, 2015, until November 14, 2022. No limit or filter was used for the time period covered or the English language, but articles were subsequently culled for the English language. Per inclusion/exclusion criteria that the task force agreed on (Table 1), studies
included for assessment were randomized controlled trials (RCTs), systematic reviews or meta-analyses of RCTs; systematic reviews or meta-analyses of a combination of RCTs, controlled trials without randomization, and cohort studies; controlled trials without randomization; cohort studies; and case-control studies. Descriptive studies, case series, case reports, letters, nonsystematic reviews, opinions on the basis of clinical experience, and reports of expert committees were excluded from this guideline. Titles and abstracts of potentially relevant articles were screened and reviewed initially according to preliminary inclusion/exclusion criteria determined by members of the task force. All task force members reviewed the articles of all citations that potentially matched the predefined selection criteria. Final inclusion or exclusion decisions were made on examination of the articles in full. Disagreements about inclusion were discussed and resolved by consensus or arbitration after consultation with an independent reviewer/epidemiologist. The search yielded 323 studies, of which 49 studies met inclusion criteria.
Table 1. Inclusion and Exclusion Criteria
| Include | Exclude |
| Randomized controlled trials (RCTs); systematic reviews or meta-analyses of RCTs; systematic reviews or meta-analyses of a combination of RCTs, controlled trials without randomization, and cohort studies; controlled trials without RCTs, controlled trials without randomization, and cohort studies; controlled trials without randomization; cohort studies; and case-control studies | Descriptive studies, case series, case reports, letters, nonsystematic reviews, opinions on the basis of clinical experience, and reports of expert committees |
| Human studies | Animal studies |
| English | Non-English |
| Studies with a comparison group | Studies without a comparison group |
| Studies that report clinical (pregnancy, live birth, miscarriage, and/or obstetrical) outcomes | Studies that focus on prevalence with no fertility and/or obstetrical outcome measures |
| Studies that focus on septate uterus | Studies that do not focus on septate uterus, but focus on unicornuate or didelphic uteri, or fibroids and polyps, or cervix and vagina, OHVIRA or HWW syndrome, Asherman, Fryns, or MRKH syndrome |
| Studies that focus on imaging modalities including but not limited to MRI, 3D ultrasound, and sonohysterography | Studies with a focus on amenorrhea, blood flow, cancer, dysmenorrhea, endometriosis, hemodynamics, menorrhagia, ovarian maldescent, polycystic ovary syndrome, surgical technique only, uterine horn, uterine prolapse, and VEGF Studies with a focus on pediatric or postpartum population Studies with a focus on abdominal metroplasty Studies that focus on embryologic development |
| 3D = 3-dimensional; HWW = Herlyn-Werner-Wunderlich; MRI = magnetic resonance imaging; MRKH = Mayer-Rokitansky-Kuster-Hauser; OHVIRA = obstructed hemivagina and ipsilateral renal anomaly; VEGF = vascular endothelial growth factor. |
|
Quality of evidence
A methodological specialist extracted data from included studies into an evidence table for outcomes identified by the task force, including live birth rate, clinical pregnancy rate, and surgical outcomes. Nonconflicted members of the task force critically assessed the strengths and limitations of available evidence that met inclusion/exclusion criteria to rate the quality of each study and assign a quality grade on the basis of the rating scale depicted in Table 2, which was recorded in the evidence table (Supplemental Table 1, available online).The task force chair reviewed grades of quality assigned by members of the task force and provided oversight throughout the entire development process. If no grade was assigned, the task force chair determined a grade of quality on the basis of a study’s strengths and limitations. The study design was evaluated, and the quality of the methodology was assessed on the basis of components including blinding, allocation concealment, appropriate control groups, intention-to-treat analysis, generalizability, and risk of bias.
The task force summarized data from the evidence table in narrative form to include the characteristics, quality, benefit, and conclusions of studies relevant to answering each treatment related to the question. The expert task force convened to review the literature and summarize findings. The task force chair presented these summaries of evidence and draft conclusions to the ASRM Practice Committee for deliberation of the strength of the evidence and the strength of the recommendations and approval of summary statements and recommendations. The quality of the evidence informed the strength of the guideline’s evidence (Table 3). Patient perspective and feedback were elicited during the review and before the publication of the guideline.
HOW TO DIAGNOSE A UTERINE SEPTUM?
For accurate differentiation of Müllerian anomalies, it is essential to visualize both the external and internal contours of the uterus (Fig. 1). As such, the historical gold standard method for diagnosing and categorizing Müllerian anomalies employed concomitant laparoscopy and hysteroscopy. With radiologic advancements over the past 30 years, the diagnosis of a septate uterus has shifted from surgical to radiographic techniques. There are several nonsurgical techniques available, including hysterosalpingography (HSG), standard 2-dimensional transvaginal ultrasound (2D TVUS), 3-dimensional TVUS with or without saline infusion, and MRI.Although HSG is often the initial test that provides evidence for a Müllerian anomaly in patients with infertility or recurrent pregnancy loss, without visualization of the external contour of the uterus, the diagnostic accuracy of the HSG is low for distinguishing septate and bicornuate uteri (8, 9). Similarly, hysteroscopy alone also cannot distinguish between these 2 anomalies. In addition, 2 studies that looked at the inter-observer diagnostic agreement of hysteroscopic videos found poor agreement among viewers (10) and only moderate improvement when standardized diagnostic criteria were employed (11).
A study of 117 female participants found that the use of 3D TVUS combined with saline infusion had 100% accuracy when compared with laparoscopy/hysteroscopy (12). In addition, 3D TVUS without saline infusion has been found to be over 88% accurate for diagnosing uterine septa in 3 studies compared with hysteroscopy/laparoscopy (12–14). Studies assessing concordance between 3D TVUS and hysteroscopy alone have shown high levels of agreement between the 2 when 3D TVUS was used first, and hysteroscopy was used as diagnostic confirmation (15,16).
Magnetic resonance imaging is often used for the diagnosis of Müllerian anomalies. Studies have shown a high level of agreement between MRI and other radiologic techniques (4, 17); however, 1 study suggests that although MRI is an accurate method to diagnose Müllerian abnormalities overall, it is only 70% accurate for the diagnosis of uterine septum (18). A study divided 63 participants with suspected uterine anomalies into 3 groups of different imaging techniques. Accuracy of Group 1 (2D TVUS and MRI), Group 2 (2D and 3D TVUS and MRI), and Group 3 (only 3D TVUS) were compared. Three-dimensional transvaginal ultrasound diagnoses, as judged by intraoperative findings, were correct in 100% of cases, whereas the MRI diagnoses in the same group were correct in only 7 of 13 cases, and laparoscopies were needed less often once 3D TVUS was introduced (19).
It must be emphasized that studies to determine how to diagnose a septum best are limited by small sample sizes and are from select centers. Therefore, it is likely that the interpretation of radiologic studies depends on the interpreter’s experience. When the diagnosis of a uterine septum is not clear, it may be helpful to seek consultation with a clinician with experience in diagnosing and managing Müllerian anomalies.
Table 2. Rating for Quality of Evidence
| Quality of evidence | Definition |
| High quality | Target population clearly identified Sufficient sample size for the study design Clear description of study design Appropriate control(s) Generalizable results Definitive conclusions Minimal risk of bias Limitations do not invalidate conclusions Evidence primarily on the basis of well-designed systematic reviews or meta-analyses of randomized controlled trials |
| Intermediate quality | Target population Sufficient sample size for the study design but could benefit from larger studies Control group identified Reasonably consistent results which limitations do not invalidate Fairly definitive conclusions Low risk of bias Evidence primarily on the basis of small randomized controlled trials; systematic reviews or meta-analyses of a combination of RCTs, controlled trials without randomization, and cohort studies; controlled trials without randomization; and/or well-designed observational studies |
| Low quality | Insufficient sample size for the study design Discrepancies among reported data Errors in study design or analysis Missing significant information Unclear or inconsistent results High risk of bias due to multiple flaws so that conclusions cannot be drawn High uncertainty about validity of conclusions |
| RCT = randomized controlled trial. | |
Summary
- Three-dimensional ultrasound with or without saline infusion has been shown to be an accurate nonsurgical method for diagnosing a uterine septum.
- Other methods including 2D US, MRI, and hysteroscopy may be useful but are less accurate.
Recommendation
- It is recommended to use 3D TVUS with or without saline infusion as the first-line noninvasive diagnostic tool in uterine shape assessment (Strength of Evidence: B; Strength of Recommendation: Moderate).
DOES A SEPTUM IMPACT FERTILITY?
The true prevalence of infertility among patients with a septate uterus is difficult to determine because many of these anomalies remain undiagnosed, given that they often do not cause any specific symptoms. Because diagnosis requires evaluation of the uterine cavity and fundal contour, most patients with this anomaly are only diagnosed when they present with conditions that require evaluation of the uterine cavity, such as a history of infertility or adverse pregnancy outcome. As a result, many studies use these patient cohorts and are only able to evaluate reproductive outcomes among patients who have already been diagnosed with infertility. Thus, our current understanding of whether a septate uterus is associated with infertility comes from studies that are limited by selection bias. One retrospective study of intermediate-quality evidence reported the incidence of septate uteri among patients with proven fertility compared with patients with infertility or recurrent pregnancy loss (20). A total of 3,181 patients who had a uterine cavity evaluation either at the time of sterilization surgery (n = 1,289) or during an evaluation for infertility or recurrent pregnancy loss (n = 1,892) were included. Among the sterilization group with proven fertility, the prevalence of a septate uterus was 1.6% (n = 20), which was not significantly different compared with the prevalence of 1.2% (n = 23) among patients with infertility or recurrent pregnancy loss (P = .43).
Table 3. Rating for Strength of Evidence
| Strength of Evidence | Definition |
| Grade A | High confidence in evidence. A larger or further study very unlikely to change the reported effect. Most of the evidence is supported by well-constructed RCTs or extremely strong and consistent observational studies with generalizable results, sufficient sample sizes for the study design, adequate controls, definitive conclusions, and minimal risk of bias. |
| Grade B | Moderate confidence in evidence. Larger or further studies are not likely to change the reported effect but may more precisely identify the magnitude of the effect. Most of the evidence comprised RCTs with potential weaknesses including small sample size or generalizability or moderately strong and consistent observational studies with reasonably consistent results, sufficient sample sizes for the study designs, identified appropriate controls, fairly definitive conclusions, and low risk of bias. |
| Grade C | Low confidence in evidence. Evidence lacking to support the reported effect. Evidence comprised observational studies with significant methodological flaws and/or inconsistent findings on the basis of poor evidence, inconsistent results, insufficient sample size for study design, conclusions that cannot be drawn, and/or high risk of bias. |
| RCT = randomized controlled trial. | |
Summary
- There is insufficient evidence to conclude whether a septate uterus is associated with infertility.
Recommendation
- No recommendation can be made regarding the association between a septate uterus and infertility due to insufficient evidence (Strength of Evidence: C; Strength of recommendation: No recommendation).
DOES A SEPTUM CONTRIBUTE TO PREGNANCY LOSS OR ADVERSE PREGNANCY OUTCOME?
There are multiple observational studies examining the relationship between uterine septum and pregnancy loss. One intermediate-quality study prospectively screened patients who presented for uterine ultrasound assessment for gynecologic symptoms but with no history of infertility or recurrent miscarriage and recorded their reproductive history and the presence of uterine anomalies (21). Among 29 patients with a septate uterus, 42% of their reported pregnancies resulted in a first-trimester spontaneous abortion, which was significantly increased compared with 12% of patients without a uterine anomaly (P<.001). The incidence of second-trimester losses was similar between the groups (3.6% [n = 2] vs. 3.5% [n = 69]). A similar association between septate uteri and first-trimester spontaneous abortion was observed in 2 intermediate-quality meta-analyses that evaluated the reproductive outcomes among patients with a septate uterus compared with those without a septate uterus (22, 23). The more recent meta-analysis included 6 studies and reported that patients with a septate uterus had a first-trimester spontaneous abortion relative risk (RR) of 2.65 (95% confidence interval [CI]: 1.39–5.06) compared with controls. In addition, a significant association was observed for second-trimester spontaneous abortion with a RR of 2.95 (95% CI: 1.51–5.77) compared with controls. An association between septate uteri and adverse obstetric outcomes beyond the second trimester has also been reported by multiple studies (20, 24–26). In addition, 3 intermediate-quality meta-analyses have assessed these outcomes (22, 23, 27). The most recent meta-analysis reported that compared with controls, pregnant patients with a septate uterus have increased odds of preterm birth (odds ratio [OR] 4.06, 95% CI: 2.89–5.70), malpresentation (OR 13.76, 95% CI: 5.52– 34.32), cesarean delivery (OR 5.19, 95% CI: 1.84–14.62), fetal growth restriction (OR 2.99, 95% CI: 1.19–7.51), and placental abruption (OR 10.70, 95% CI: 4.01–28.53) (24).Summary
- There is good evidence that a septate uterus is associated with spontaneous abortion.
- There is good evidence that a septate uterus is associated with preterm birth, malpresentation, and cesarean delivery.
- There is fair evidence that a septate uterus is associated with placental abruption and fetal growth restriction.
Recommendation
- It is recommended to counsel patients that the presence of a septate uterus is associated with spontaneous abortion and obstetric complications (Strength of Evidence: B; Strength of Recommendation: Moderate).
DOES TREATING A SEPTUM IMPROVE FERTILITY IN INFERTILE PATIENTS?
Despite the absence of evidence linking the presence of a uterine septum with infertility, numerous studies have addressed the question of whether uterine septum incision has a beneficial effect on subsequent fertility and pregnancy outcomes. Until recently, all studies on this topic were observational (25). Most observational studies were case series, which reported on pregnancy rates among infertile patients after septoplasty (26–33). Such studies often contain methodological flaws and are prone to selection bias and regression to the mean.In 1 such study, 33 of 72 participants (45.83%) with a septate uterus and otherwise unexplained primary infertility were conceived within 1 year of surgery (26). In another, 88 patients with primary unexplained infertility for over 2 years and a uterine septum were prospectively observed after hysteroscopic septoplasty (28), 41% of the patients conceived with a median time to conception of 7.5 ± 2.6 months.
There are a few cohort studies. In 1 prospective study, 44 participants with a septate uterus and no other causes of infertility were compared with 132 patients with unexplained infertility (34). The septum group was initially treated with hysteroscopic septum incision, and both groups were followed expectantly for 1 year. At 12 months, the pregnancy rate for the septum group was 38.6% compared with 20.4% in the unexplained infertility-only group, with live birth rates of 34.1% and 18.9%, respectively (P<.05). In another study involving 127 patients diagnosed with unexplained infertility and a uterine septum, 102 patients who chose to undergo hysteroscopic metroplasty were compared with 25 who chose not to undergo the operation (35). Pregnancy (43.1% vs. 20%) and live birth rates (35.3% vs. 8%) were significantly higher in the group choosing to undergo surgery (P>.05), despite no significant differences in age, body mass index, duration of infertility or septum classification.
Several studies attempted to answer the question of whether hysteroscopic septoplasty is indicated before in vitro fertilization (36–38). One such study evaluated embryo transfer outcomes in patients with an untreated uterine septum (n = 289), patients treated with hysteroscopic septum incision (n = 538), and matched controls without a history of a uterine anomaly (n = 1,654) (38). Pregnancy (12.4% vs. 29.2%) and live birth rates (2.7% vs. 21.7%) were significantly lower in patients with an untreated uterine septum compared with matched controls (P<.05). Pregnancy and live birth rates in patients who had undergone septoplasty were not significantly different compared with controls (22.9% vs. 26.0% and 15.6% vs. 20.9%, respectively; not significant). In a multivariate logistic regression analysis, septum incision before embryo transfer was an independent predictor of pregnancy (OR 2.507, 95% CI: 1.539–4.111, P<.001).
In the first RCT to assess reproductive outcomes related to a septate uterus, 80 participants with a septate uterus and a history of either infertility, pregnancy loss, or preterm birth were randomized to septum incision (n = 40) or expectant management (n = 40) and observed for the primary outcome of conception leading to live birth within 12 months after randomization (5). Live birth occurred in 12 of 39 participants in the septoplasty group (31%) and in 14 of 40 participants allocated to expectant management (35%) (RR 0.88, 95% CI: 0.47–1.65). There was 1 uterine perforation in a patient allocated to septum incision (1/39 = 2.6%). The recruitment period for this multicenter international trial of high quality was long, and the sample size was limited.
In the face of conflicting evidence from numerous lower quality studies demonstrating a benefit of septum incision and 1 RCT of limited sample size demonstrating no benefit, patients with infertility and a uterine septum should be counseled about the limitations of the literature and the option of undergoing septum incision in a shared decision-making model.
Summary
- Low-quality data suggest that surgical correction of a uterine septum may improve fertility in patients with unexplained infertility. One prospective RCT with a limited sample size did not demonstrate improvement in live birth rate.
Recommendation
- Although septum incision in patients with infertility and/or undergoing fertility treatment is reasonable, a firm recommendation for this practice cannot be made on the basis of the current evidence.
- It is recommended to counsel patients with infertility and/or undergoing fertility treatment that resection of the septum may or may not be associated with an increase in live births. Given limitations in the literature and low risk of the procedure, septum incision may be offered to patients in a shared decision-making model (Strength of Evidence: B; Strength of Recommendation: Moderate).
DOES TREATING A SEPTUM IMPROVE OBSTETRICAL OUTCOMES?
Numerous retrospective studies and 1 prospective randomized trial sought to evaluate pregnancy outcomes after septum incision. Significant heterogeneity exists between and within the retrospective studies, with variable indications for surgery.Many published studies follow a simple ‘‘before–after’’ design with reported pregnancy outcomes before and after the procedure and patients serving as their own controls. These low-quality studies have demonstrated an improvement in the assessed outcomes, including pregnancy loss and a variety of obstetric outcomes such as preterm delivery, fetal malpresentation, and cesarean section (30–32, 39–44).
The available retrospective studies with a comparison group have varied in the exact study question and design. Although some compared patients undergoing surgical correction of a septum with those without a history of uterine anomaly (38, 45, 46), others aimed to investigate differences in outcomes according to the type of uterine anomaly (arcuate, subseptate, and septate) and/or septum size (33, 47–49). In 1 study in the ART setting including 420 participants with an arcuate uterus (Group A) and 406 participants with a septate or subseptate uterus (Group B), the preterm birth rates before and after septum incision decreased similarly in both groups: 33.9% before and 7.2% after in Group A vs. 36.5% before and 8.0% after in Group B 50). One study including 73 patients with infertility undergoing hysteroscopic metroplasty found that compared with participants with an incomplete septum, those with a complete septum had a lower rate of miscarriage, but also a lower mean gestational age at delivery and infant birth weight after surgical correction (50). An international retrospective cohort study published in 2020 assessed 257 individuals with septate uterus in 21 centers in the Netherlands, the United States, and the United Kingdom. The participants were allocated to resection of septum vs. expectant management on the basis of reproductive history and severity of disease at the discretion of the treating physician. In total, 151 participants underwent septum resection, and 106 had expectant management; no significant difference in a live birth (53% vs. 71%, respectively, hazard ratio 0.71, 95% CI: 0.49–1.02), pregnancy loss (46.8% vs. 34.4%, respectively, OR 1.58, 95% CI: 0.81–3.09) or preterm birth (29.2% vs. 16.7%, respectively, OR 1.26, 95% CI: 0.52–3.04) was demonstrated. There was a significant decrease in malpresentation in patients who underwent septum resection compared with expectant management (19.1% vs. 34.6%, respectively, OR 0.56 95% CI: 0.24–1.33.) It should be noted that classification of septum changed over the study period ranging from 2000 to 2018 and patients with arcuate uterus included in the expectant management group which may have contributed to selection bias and contributed to improved outcomes reported in the expectant management group (51).
A variety of meta-analyses on this topic aimed to pool retrospective studies comparing patients undergoing surgical septum correction with a control group of patients with a uterine septum who were managed expectantly (2, 22, 50, 52). The most recent of these (50) also included the only prospective randomized trial on the topic (5), which demonstrated no difference in live birth in participants randomized to septum incision (n = 40) and those allocated to expectant management (n = 40) in a population with a septate uterus and a history of either infertility, pregnancy loss or preterm birth (live birth rates 31% vs. 35%; RR 0.88; 95% CI: 0.47–1.65). The study (5) was terminated early due to poor recruitment and was therefore underpowered to detect the prespecified endpoints.
In addition to the RCT, 10 observational studies met the inclusion criterion of comparing patients undergoing hysteroscopic septum incision to expectant management (50). For the 1,589 participants included in the meta-analysis, a statistically significant reduction in the rate of miscarriage in those undergoing septum correction was noted overall (pooled OR 0.45; 95% CI: 0.22–0.90); as well as in the subgroup analyses of those with a complete septum (pooled OR 0.16; 95% CI: 0.03–0.78) and those with a partial septum (pooled OR 0.36; 95% CI: 0.19–0.71). In addition, the risk of fetal malpresentation was significantly reduced (OR = 0.32, 95% CI: 0.16–0.65). For the subgroup of participants who underwent surgical correction of a partial septum, a significant decrease in the frequency of preterm birth was found compared with patients managed expectantly (OR = 0.30, 95% CI: 0.11–0.79). Overall, no significant differences were found between the 2 groups in the likelihood of clinical pregnancy, term live birth, or risk of cesarean delivery (50).
Summary
- Surgical correction of a uterine septum in patients with a history of poor reproductive outcomes appears to be associated with a lower rate of miscarriage.
- On the basis of limited observational data, surgical correction of a uterine septum appears to improve obstetric outcomes, including abnormal fetal presentation, preterm delivery, and the rate of cesarean section. However, no effect on the live birth rate has been demonstrated.
Recommendation
- It is recommended to offer hysteroscopic septum incision to patients with a septum and a history of recurrent miscarriage in a shared decision-making model (Strength of Evidence: B; Strength of Recommendation: Moderate).
- It is recommended to counsel patients that septum incision may decrease the risk of adverse obstetric outcomes such as malpresentation and cesarean section but there are no high-quality data to recommend this practice (Strength of Evidence: B; Strength of Recommendation: Moderate).
ARE SEPTUM CHARACTERISTICS ASSOCIATED WITH REPRODUCTIVE OUTCOMES?
Uterine septa comprise myometrium similar to the normal myometrium in the remainder of the uterus (53, 54), and the presence of a muscular septum is associated with an increased risk of recurrent miscarriage and poor pregnancy outcomes. Although the exact mechanism of these poor reproductive outcomes is unknown, it is logical to expect the larger complete septa to produce more adverse events than the smaller partial septa. No prospective trials specifically address this question. All available data are in the form of retrospective case-controlled trials that examined the reproductive outcomes after metroplasty for complete and partial septa. Tomazevic et al. (38) retrospectively reviewed over 2,400 embryos transferred in patients with complete septa, partial septa, and arcuate uteri compared with normal controls and found a lower implantation rate and live birth rate in all 3 groups compared with controls. These differences from controls were eliminated in all 3 categories after metroplasty (52). Several smaller retrospective studies concluded an equal reduction in miscarriage rate after metroplasty of small and large septa (29, 33, 37). Our conclusion is that there was no difference in outcomes after resection of a small vs. large septa.Summary
- All available data are in the form of retrospective case-controlled trials. Most studies evaluated the early pregnancy loss incidence in patients before and after surgical correction.
- Patients with recurrent pregnancy loss demonstrated similar benefits after resection of small and large septa.
Recommendation
- It is not recommended to use the size or shape of a septum to determine the impact on adverse reproductive outcomes (Strength of Evidence: B/C; Strength of recommendation: Moderate/Weak).
SHOULD PREOPERATIVE MANAGEMENT TO THIN THE ENDOMETRIUM BE USED?
There are no high-quality data examining the benefits or risks of preoperative adjuvants such as oral contraceptive pills or gonadotropin-releasing hormone agonists that may enhance intrauterine visualization but also disrupt the normal hormonal milieu, which can affect postsurgical healing. It is important to have adequate visualization to see both tubal ostia when transecting a septum. This can be achieved by operating in the early follicular phase or after progesterone withdrawal in patients with irregular ovulation or by placing patients on oral contraceptives to regulate the menstrual cycle and schedule the operative procedure.Summary
- There are no high-quality studies designed to evaluate whether or not there is a benefit for preoperative hormonal suppression before incising a uterine septum.
Recommendation
- It is recommended, on the basis of expert committee opinion, to consider performing the procedure during the follicular phase or after progesterone withdrawal to help with visualization during surgery. However, there are no studies designed to prove or disprove this (Strength of Evidence: C; Strength of recommendation: Weak).
ARE THERE ANY RISKS OF CERVICAL INSUFFICENCY BY RESECTING THE CERVICAL PORTION OF THE SEPTUM?
A complete uterine septum extends from the fundus to the level of the external cervical os. Historically, it has been controversial as to whether the surgeon should incise the cervical portion of the septum or start the incision at the level of the internal cervical os and leave the cervical portion intact. Concerns for cervical septum removal include intraoperative bleeding and future cervical incompetence, with the potential benefit of more efficient, less complicated surgery. Three studies have evaluated these questions. One clinical trial randomized 28 participants with a complete uterine septum to septoplasty, including the unicollis cervical septum compared with septoplasty with cervical preservation. There were no differences in reproductive outcomes such as early and late abortion and preterm delivery between groups with significantly faster operative times when the unicollis cervical septum was removed. In addition, there were 2 cases of pulmonary edema and 3 cases of significant bleeding (>150 mL) in the cervical preservation group (55). Two other small prospective studies of patients who underwent complete septum incision, including cervical septoplasty, found no significant bleeding and no evidence of cervical incompetence (56) and shorter operative times when compared with historical controls (56).Summary
- Incision of a unicollis cervical septum leads to faster operative times and less fluid deficits.
- One RCT showed an improved safety and efficiency profile with resection of the unicollis cervical septum.
- No adverse reproductive outcomes were reported in these 3 studies.
- No cases of cervical insufficiency were reported in these studies.
Recommendation
- It is recommended to counsel patients that, on the basis of limited data, there is no evidence that resection of the unicollis cervical septum increases the risk of cervical insufficiency (Strength of Evidence: C; Strength of recommendation: Weak).
IS THERE A BENEFIT TO COMPLETE EXCISION OF RESIDUAL (<10 MM) SEPTUM?
When transecting a uterine septum, the surgeon must decide if the goal is to create a flat fundus between the 2 tubal ostia, to transect only until what appears to be normal vasculature is identified, or to leave an ‘‘arcuate’’ shape that is not felt to be associated with poor reproductive outcomes. Although the data available are from 1 retrospective study with 72 patients, the results suggest that there is no difference in reproductive outcomes when a small residual septum is left in place vs. complete removal of the septum (57).Reproductive outcome in 17 patients with a residual septum of between 0.5 and 1 cm after hysteroscopic metroplasty was compared with that in 51 patients with no residual septum or one of <0.5 cm. Septal surgery was performed with scissors or a resectoscope. The cumulative 18-month probability of becoming pregnant was 44.5% in the patients with a residual septum, and 52.7% in those with no residual septum (not significantly different), and the cumulative 18-month probability of giving birth to a child was 27.5% and 36%, respectively (not significant).
It is recommended that the uterine septum should be transected with the goal of restoring normal anatomy. However, leaving an arcuate shape due to observed normal muscular vasculature does not appear to reduce the benefit of the metroplasty.
Summary
- There is only 1 study on the impact of a residual septum. Limited data suggest that there is no difference in reproductive outcomes when a small residual septum (<1 cm) is left in place vs. complete removal of the septum.
Recommendation
- It is not recommended to perform another surgery for a residual septum under 1 cm (Strength of Evidence: C; Strength of recommendation: Weak).
IS ADHESION PREVENTION NEEDED?
Uterine septa arise from the incomplete resorption of uterine muscular tissue during the unification of the uterine horns in utero. Proper surgical correction of the congenital malformation involves incising the midline of the septa. Septal tissue should not be resected or removed. After the septum incision, there is natural tension to retract the tissue toward the anterior and posterior uterine walls. In theory, a septum incision with mechanical energy (cold scissors) should minimize the risk of damage to normal endometrial tissue compared with thermal energy with electrosurgery. However, there is no high-quality data to support one modality over another. There is a concern that the septum incision will lead to intrauterine scar tissue or septa reformation. The question is, what is the incidence of intrauterine adhesions after metroplasty, and if the use of adjuvants such as high doses of estrogen, intrauterine balloons, or intrauterine devices (IUDs) will reduce the risk of post metroplasty adhesion formation? Prospective RCTs have shown no benefit to postoperative treatment with either an intrauterine balloon (58) or oral estrogen (59), whereas retrospective studies have shown no benefit of estrogen therapies or the placement of IUDs after septum incision (60–62). The use of auto-crosslinked polysaccharide gel has been shown in 1 study to reduce postseptum incision adhesion formation (63). This gel is currently unavailable in the US and warrants further investigation.Summary
- Several studies were designed to evaluate the effectiveness of postprocedural therapy to reduce adhesion formation. The studies evaluated oral estrogen, intrauterine balloons and IUDs and 1 study evaluated a dissolvable gel that is not available in the US.
- There are no high-quality data to demonstrate the benefit of postoperative estrogen therapy, IUDs, or intrauterine balloons to prevent intrauterine adhesions postmetroplasty. The data on the value of intrauterine gels are too limited to draw conclusions.
Recommendation
- There is insufficient evidence to recommend routine administration of oral estrogen, intrauterine balloons and IUDs to decrease adhesion formation after septoplasty (Strength of Evidence: C; Strength of recommendation: Weak).
IS THERE AN INCREASED RISK OF UTERINE RUPTURE IN A PREGNANCY AFTER A HYSTEROSCOPIC RESECTION OF A SEPTUM?
There have been few case reports in the literature of uterine rupture during pregnancy or delivery after septum incision. According to a meta-analysis of reported ruptures, the risk of subsequent pregnancy-related uterine rupture is correlated with excessive septal excision, penetration of the myometrium, uterine wall perforation, and excessive use of cautery or laser energy during the initial septum incision procedure (2). A Belgium nationwide population-based cohort study of uterine rupture found only 2 of 90 ruptures occurred in patients who had undergone previous septoplasty (in comparison with 73 with a prior c-section), with an overall very low rupture rate in the population (64). Although uterine rupture is rarely reported in the available literature on septoplasty outcomes, in 1 study where it was a reported outcome, there were no reports of uterine rupture in the 75 patients who underwent septoplasty (65).Summary
- There is a paucity of data limited to case reports and rare outcomes in population studies of uterine rupture after septoplasty.
Recommendation
- It appears the rate of uterine rupture after septoplasty is rare, however, this outcome is not often reported on in the current literature (Strength of Evidence: B/C; Strength of recommendation: Insufficient data to make a recommendation).
HOW LONG AFTER SURGICAL TREATMENT OF A UTERINE SEPTUM SHOULD A PATIENT WAIT TO CONCEIVE?
The time from septum incision to attempting pregnancy has not been evaluated in randomized controlled studies. However, A few studies address uterine healing after surgical treatment of a septum. One study assessed the postoperative appearance of the endometrium and correlated this with endometrial biopsy specimens in 19 participants who were randomized to follow-up hysteroscopy at 1, 2, 4, or 8 weeks after hysteroscopic septum incision (64). At 2 weeks postoperatively, the incised zone of the septum was depressed on both uterine walls and had wide areas lacking endometrial covering. By 8 weeks postoperatively, the uterine cavity was morphologically normal, and the covering endometrium was regular. Another prospective study evaluated 16 patients with office hysteroscopy every 2 weeks after hysteroscopic septum incision until wound healing was complete (65). After septum incision, 19% of patients at 1 month and 100% of patients by 2 months postoperatively demonstrated a healed uterine cavity.A single retrospective cohort study evaluated pregnancy rates in 282 patients after in vitro fertilization/intracytoplasmic sperm injection when the embryo transfer was performed within 9 weeks, between 10 and 16 weeks, and 17+ weeks after uterine septum incision. Pregnancy rates and miscarriage rates were no different among the 3 groups (66).
Summary
- There are only a few low- to intermediate-quality studies addressing this question, but it appears that embryo transfer 1–2 months after septoplasty has similar reproductive outcomes to waiting >2 months.
- There are no data to indicate that patients should wait longer than 1–2 months to try to conceive after hysteroscopic septoplasty.
Recommendation
- It is recommended to counsel patients that they may proceed with fertility treatment in 1–2 months after septoplasty (Strength of Evidence: C; Strength of recommendation: Weak).
HOW SHOULD AN INCIDENTALLY DISCOVERED SEPTUM BE MANAGED IN A PATIENT WHO IS NOT (YET) TRYING TO CONCEIVE?
With improvements in noninvasive pelvic imaging and lower thresholds for obtaining imaging for complaints such as abdominal pain, there is a growing subset of patients with incidentally diagnosed uterine septum. There have been no randomized studies to date to evaluate if uterine septoplasty improves reproductive outcomes for patients before attempting conception.Summary
- There are no data addressing this question.
Recommendation
- There is insufficient evidence to recommend hysteroscopic septoplasty in patients who have not yet attempted conception (Strength of Evidence: Insufficient Strength of recommendation: Insufficient evidence to make recommendation).
Acknowledgments
The Practice Committee acknowledges the special contributions of the following members of the ASRM Practice Committee who participated in the development and review of this document:
Review process
This report was developed under the direction of the Practice Committee of the American Society for Reproductive Medicine as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or to dictate an exclusive course of treatment. Other plans of management may be appropriate, taking into account the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice Committee and the Board of Directors of the American Society for Reproductive Medicine have approved this report.This document was reviewed by ASRM members and their input was considered in the preparation of the final document. The following members of the ASRM Practice Committee participated in the development of this document: Alan Penzias, M.D.; Paula Amato, M.D.; Jacob Anderson; Kristin Bendikson, M.D.; Clarisa Gracia, M.D., M.S.C.E.; Tommaso Falcone, M.D.; Rebecca Flyckt, M.D.; Karl Hansen, M.D., Ph.D.; Micah Hill, D.O.; Sangita Jindal, Ph.D.; Suleena Kalra, M.D., M.S.C.E.; Tarun Jain, M.D.; Bruce Pier, M.D.; Michael Thomas, M.D.; Richard Reindollar, M.D.; Jared Robins, M.D.; Chevis N. Shannon, Dr.Ph., M.B.A., M.P.H.; Anne Steiner, M.D., M.P.H.: Cigdem Tanrikut, M.D.; and Belinda Yauger, M.D. The Practice Committee acknowledges the special contribution of Tommaso Falcone, M.D.; Jessica Goldstein, R.N.; Jeffrey Hayes, Ph.D.; Keith Isaacson, M.D.; Linnea Goodman, M.D.; Alex Quaas, M.D.; and Phillip Romanski, M.D. in the preparation of this document. All Committee members disclosed commercial and financial relationships with manufacturers or distributors of goods or services used to treat patients. Members of the Committee who were found to have conflicts of interest on the basis of the relationships disclosed did not participate in the discussion or development of this document.
Patient/public perspective
To incorporate the perspectives of those who might be affected most by the recommendations in this guideline, a group of patient volunteers and lay stakeholders in reproductive medicine who were not involved in the scoping or development of this guideline reviewed the document. Their feedback was considered in the preparation of the final document.
Funding
This guideline was developed with financial support from the American Society for Reproductive Medicine (ASRM). Investigators who serve on the ASRM Practice Committee were reimbursed by ASRM for expenses related to travel to Practice Committee meetings where they reviewed drafts of manuscripts. ASRM receives no outside funding for the development of guidelines.
Updating policy
This document will be reviewed for currency within 5 years of publication.
Panel
This evidence-based guideline with recommendations for clinicians was developed by a multidisciplinary group, comprising the ASRM Practice Committee and a task force of medical experts, which included specialists in obstetrics and gynecology, reproductive endocrinology and infertility, fertility preservation, reproductive surgery, endometriosis, uterine anomalies, fibroids, assisted reproductive technology, in vitro fertilization, and epidemiology/biostatistics. Members of the task force for this clinical practice guideline consisted of medical professionals at various levels of training, including fellows and senior experts, as well as experts with <10 years of posttraining, CREST (Clinical Reproductive Scientist Training) Program scholars, a clinical epidemiologist who is also a reproductive medicine subspecialist, and a methodologic specialist. In addition, a select group of patients participated in document scoping and review.
Disclaimer
This report was developed under the direction of the Practice Committee of the American Society for Reproductive Medicine (ASRM) as a service to its members and other practicing clinicians. Although this document reflects appropriate management of a problem encountered in the practice of reproductive medicine, it is not intended to be the only approved standard of practice or to dictate an exclusive course of treatment. Other plans of management may be appropriate, taking into account the needs of the individual patient, available resources, and institutional or clinical practice limitations. The Practice Committee and the Board of Directors of the American Society for Reproductive Medicine have approved this report.
Declaration of Interests
Per ASRM policy, all members of ASRM task forces and the Practice Committee disclosed commercial and financial relationships with manufacturers or distributors of goods or services used to treat patients for the preceding 12 months. Committee members were reminded to update potential disclosures annually and if new potential conflicts arose during their appointments. Before live discussions or meetings, Committee members were reminded verbally and in writing to disclose any new or previously undisclosed relationships. Disclosures were reviewed for conflicts by the ASRM Chief Medical Officer and the Chair of the Practice Committee. Task force members for whom conflicts were identified were excused from this project. Members of the Practice Committee who were found to have conflicts of interest on the basis of the relationships disclosed did not participate in the discussion or development of the document.
REFERENCES
- Saravelos SH, Cocksedge KA, Li TC. Prevalence and diagnosis of congenital uterine anomalies in women with reproductive failure: a critical appraisal. Hum Reprod Update 2008;14:415–29.
- Valle RF, Ekpo GE. Hysteroscopic metroplasty for the septate uterus: review and meta-analysis. J Minim Invasive Gynecol 2013;20:22–42.
- Dabirashrafi H, Bahadori M, Mohammad K, Alavi M, Moghadami-Tabrizi N, Zandinejad K, et al. Septate uterus: new idea on the histologic features of the septum in this abnormal uterus. Am J Obstet Gynecol 1995;172:105–7.
- Pellerito JS, McCarthy SM, Doyle MB, Glickman MG, DeCherney AH. Diagnosis of uterine anomalies: relative accuracy of MR imaging, endovaginal sonography, and hysterosalpingography. Radiology 1992;183:795–800.
- Rikken JFW, Kowalik CR, Emanuel MH, Bongers MY, Spinder T, Jansen FW, et al. Septum resection versus expectant management in women with a septate uterus: an international multicentre open-label randomized controlled trial. Hum Reprod 2021;36:1260–7.
- Oppelt P, Renner SP, Brucker S, Strissel PL, Strick R, Oppelt PG, et al. The VCUAM (Vagina Cervix Uterus Adnex-associated Malformation) classification: a new classification for genital malformations. Fertil Steril 2005;84: 1493–7.
- American Fertility Society. The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, mullerian anomalies and intrauterine adhesions. Fertil Steril 1988;49:944–55.
- Braun P, Grau FV, Pons RM, Enguix DP. Is hysterosalpingography able to diagnose all uterine malformations correctly? A retrospective study. Eur J Radiol 2005;53:274–9.
- Sheth SS, Sonkawde R. Uterine septum misdiagnosed on hysterosalpingogram. Int J Gynaecol Obstet 2000;69:261–3.
- Smit JG, Kasius JC, Eijkemans MJ, Veersema S, Fatemi HM, Santbrink Van EJ, et al. The international agreement study on the diagnosis of the septate uterus at office hysteroscopy in infertile patients. Fertil Steril 2013;99: 2108–21013.e2.
- Smit JG, Overdijkink S, Mol BW, Kasius JC, Torrance HL, Eijkemans MJ, et al. The impact of diagnostic criteria on the reproducibility of the hysteroscopic diagnosis of the septate uterus: a randomized controlled trial. Hum Reprod 2015;30:1323–30.
- Ludwin A, Pitynski K, Ludwin I, Banas T, Knafel A. Two- and three-dimensional ultrasonography and sonohysterography versus hysteroscopy with laparoscopy in the differential diagnosis of septate, bicornuate, and arcuate uteri. J Minim Invasive Gynecol 2013;20:90–9.
- Moini A, Mohammadi S, Hosseini R, Eslami B, Ahmadi F. Accuracy of 3-dimensional sonography for diagnosis and classification of congenital uterine anomalies. J Ultrasound Med 2013;32:923–7.
- Faivre E, Fernandez H, Deffieux X, Gervaise A, Frydman R, Levaillant JM. Accuracy of three-dimensional ultrasonography in differential diagnosis of septate and bicornuate uterus compared with office hysteroscopy and pelvic magnetic resonance imaging. J Minim Invasive Gynecol 2012;19:101–6.
- Lagana AS, Ciancimino L, Mancuso A, Chiofalo B, Rizzo P, Triolo O. 3D sonohysterography vs hysteroscopy: a cross-sectional study for the evaluation of endouterine diseases. Arch Gynecol Obstet 2014;290:1173–8.
- Loverro G, Nappi L, Vicino M, Carriero C, Vimercati A, Selvaggi L. Uterine cavity assessment in infertile women: comparison of transvaginal sonography and hysteroscopy. Eur J Obstet Gynecol Reprod Biol 2001;100:67–71.
- Bermejo C, Martínez Ten P, Cantarero R, Diaz D, Perez Pedregosa J, Barron E, et al. Three-dimensional ultrasound in the diagnosis of Mullerian duct anomalies and concordance with magnetic resonance imaging. Ultrasound Obstet Gynecol 2010;35:593–601.
- Mueller GC, Hussain HK, Smith YR, Quint EH, Carlos RC, Johnson TD, et al. Mullerian duct anomalies: comparison of MRI diagnosis and clinical diagnosis. Am J Roentgenol 2007;189:1294 302.
- Imboden S, Muller M, Raio L, Mueller MD, Tutschek B. Clinical significance of 3D ultrasound compared to MRI in uterine malformations. Ultraschall Med 2014;35:440–4.
- Raga F, Bauset C, Remohi J, Bonilla-Musoles F, Simon C, Pellicer A. Reproductive impact of congenital Mullerian anomalies. Hum Reprod 1997;12:2277–81.
- Woelfer B, Salim R, Banerjee S, Elson J, Regan L, Jurkovic D. Reproductive outcomes in women with congenital uterine anomalies detected by three-dimensional ultrasound screening. Obstet Gynecol 2001;98:1099–103.
- Venetis CA, Papadopoulos SP, Campo R, Gordts S, Tarlatzis BC, Grimbizis GF. Clinical implications of congenital uterine anomalies: a meta-analysis of comparative studies. Reprod Biomed Online 2014;29:665–83.
- Chan YY, Jayaprakasan K, Tan A, Thornton JG, Coomarasamy A, Raine-Fenning NJ. Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound Obstet Gynecol 2011;38:371–82.
- Panagiotopoulos M, Tseke P, Michala L. Obstetric complications in women with congenital uterine anomalies according to the 2013 European Society of Human Reproduction and Embryology and the European Society for Gynaecological Endoscopy Classification: a systematic review and meta-analysis. Obstet Gynecol 2022;139:138–48.
- Rikken JF, Kowalik CR, Emanuel MH, Mol BW, van der Veen F, van Wely M, et al. Septum resection for women of reproductive age with a septate uterus. Cochrane Database Syst Rev 2017;1:CD008576.
- Dalal RJ, Pai HD, Palshetkar NP, Takhtani M, Pai RD, Saxena N. Hysteroscopic metroplasty in women with primary infertility and septate uterus: reproductive performance after surgery. J Reprod Med 2012;57:13–6.
- Pabuccu R, Gomel V. Reproductive outcome after hysteroscopic metroplasty in women with septate uterus and otherwise unexplained infertility. Fertil Steril 2004;81:1675–8.
- Shokeir T, Abdelshaheed M, El-Shafie M, Sherif L, Badawy A. Determinants of fertility and reproductive success after hysteroscopic septoplasty for women with unexplained primary infertility: a prospective analysis of 88 cases. Eur J Obstet Gynecol Reprod Biol 2011;155:54–7.
- Bendifallah S, Faivre E, Legendre G, Deffieux X, Fernandez H. Metroplasty for AFS Class V and VI septate uterus in patients with infertility or miscarriage: reproductive outcomes study. J Minim Invasive Gynecol 2013;20:178–84.
- Gundabattula SR, Joseph E, Marakani LR, Dasari S, Nirmalan PK. Reproductive outcomes after resection of intrauterine septum. J Obstet Gynaecol 2014;34:235–7.
- Saygili-Yilmaz E, Yildiz S, Erman-Akar M, Akyuz G, Yilmaz Z. Reproductive outcome of septate uterus after hysteroscopic metroplasty. Arch Gynecol Obstet 2003;268:289–92.
- Jakiel G, Robak-Cho1ubek D, Przytu1a-Pi1at M. Two-year studies of women with fertility problems following uterine septum hysteroscopic treatment. Ann Univ Mariae Curie Sklodowska Med 2004;59:65–9.
- Karadag B, Dilbaz B, Demir B, Ozgurluk I, Kocak M, Karasu Y, et al. Reproductive performance after hysteroscopic metroplasty in infertile women: complete versus partial uterine septum. Clin Exp Obstet Gynecol 2016;43:584–7.
- Mollo A, De Franciscis P, Colacurci N, Cobellis L, Perino A, Venezia R, et al. Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial. Fertil Steril 2009;91:2628–31.
- Tonguc EA, Var T, Batioglu S. Hysteroscopic metroplasty in patients with a uterine septum and otherwise unexplained infertility. Int J Gynaecol Obstet 2011;113:128–30.
- Ozgur K, Isikoglu M, Donmez L, Oehninger S. Is hysteroscopic correction of an incomplete uterine septum justified prior to IVF? Reprod Biomed Online 2007;14:335–40.
- Ban-Frangez H, Tomazevic T, Virant-Klun I, Verdenik I, Ribic-Pucelj M, Bokal EV. The outcome of singleton pregnancies after IVF/ICSI in women before and after hysteroscopic resection of a uterine septum compared to normal controls. Eur J Obstet Gynecol Reprod Biol 2009;146:184–7.
- Tomazevic T, Ban-Frangez H, Virant-Klun I, Verdenik I, Pozlep B, Vrtacnik-Bokal E. Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in IVF/ICSI. Reprod Biomed Online 2010;21:700–5.
- Freud A, Harlev A, Weintraub AY, Ohana E, Sheiner E. Reproductive outcomes following uterine septum resection. J Matern Fetal Neonatal Med 2015;28:2141–4.
- Grynberg M, Gervaise A, Faivre E, Deffieux X, Frydman R, Fernandez H. Treatment of twenty-two patients with complete uterine and vaginal septum. J Minim Invasive Gynecol 2012;19:34–9.
- Sendag F, Mermer T, Yucebilgin S, Oztekin K, Bilgin O. Reproductive outcomes after hysteroscopic metroplasty for uterine septum. Clin Exp Obstet Gynecol 2010;37:287–9.
- Valli E, Vaquero E, Lazzarin N, Caserta D, Marconi D, Zupi E. Hysteroscopic metroplasty improves gestational outcome in women with recurrent spontaneous abortion. J Am Assoc Gynecol Laparosc 2004;11:240–4.
- Wang Z, An J, Su Y, Liu C, Lin S, Zhang J, et al. Reproductive outcome of a complete septate uterus after hysteroscopic metroplasty. J Int Med Res 2020;48:300060519893836.
- Zlopasa G, Skrablin S, Kalafatic D, Banovic V, Lesin J. Uterine anomalies and pregnancy outcome following resectoscope metroplasty. Int J Gynaecol Obstet 2007;98:129–33.
- Loddo A, D'alterio MN, Neri M, Masala F, Cane FL, Melis GB. Pregnancy complications after hysteroscopic metroplasty: a ten-year case-control study. Surg Technol Int 2017;30:205–9.
- Ozgur K, Bulut H, Berkkanoglu M, Coetzee K. Perinatal outcomes in singleton and twin ICSI pregnancies following hysteroscopic correction of partial intrauterine septa. J Assist Reprod Genet 2015;32:533–41.
- Wang X, Hou H, Yu Q. Fertility and pregnancy outcomes following hysteroscopic metroplasty of different sized uterine septa: a retrospective cohort study protocol. Med (Baltim) 2019;98:e16623.
- Sukur YE, Yakistıran B, Ozmen B, Sonmezer M, Berker B, Atabekoglu C. Hysteroscopic corrections for complete septate and T-shaped uteri have similar surgical and reproductive outcome. Reprod Sci 2018;25:1649–54.
- Tomazevic T, Ban-Frangez H, Ribic-Pucelj M, Premru-Srsen T, Verdenik I. Small uterine septum is an important risk variable for preterm birth. Eur J Obstet Gynecol Reprod Biol 2007;135:1547.
- Carrera M, Perez Millan F, Alcazar JL, Alonso L, Caballero M, Carugno J, et al. Effect of hysteroscopic metroplasty on reproductive outcomes in women with septate uterus: systematic review and meta-analysis. J Minim Invasive Gynecol 2022;29:465–75.
- Rikken JFW, Verhorstert KWJ, Emanuel MH, Bongers MY, Spinder T, Kuchenbecker W, et al. Septum resection in women with a septate uterus: a cohort study. Hum Reprod 2020;35:1578–88.
- Krishnan M, Narice BF, Ola B, Metwally M. Does hysteroscopic resection of uterine septum improve reproductive outcomes: a systematic review and meta-analysis. Arch Gynecol Obstet 2021;303:1131–42.
- Sparac V, Kupesic S, Ilijas M, Zodan T, Kurjak A. Histologic architecture and vascularization of hysteroscopically excised intrauterine septa. J Am Assoc Gynecol Laparosc 2001;8:111–6.
- Rikken J, Leeuwis-Fedorovich NE, Letteboer S, Emanuel MH, Limpens J, van der Veen F, et al. The pathophysiology of the septate uterus: a systematic review. BJOG 2019;126:1192–9.
- Parsanezhad ME, Alborzi S, Zarei A, Dehbashi S, Shirazi LG, Rajaeefard A, et al. Hysteroscopic metroplasty of the complete uterine septum, duplicate cervix, and vaginal septum. Fertil Steril 2006;85:1473–7.
- Vercellini P, Ragni G, Trespidi L, Oldani S, Panazza S, Crosignani PG. A modified technique for correction of the complete septate uterus. Acta Obstet Gynecol Scand 1994;73:425–8.
- Fedele L, Bianchi S, Marchini M, Mezzopane R, Di Nola G, Tozzi L. Residual uterine septum of less than 1 cm after hysteroscopic metroplasty does not impair reproductive outcome. Hum Reprod 1996;11:727–9.
- Abu Rafea BF, Vilos GA, Oraif AM, Power SG, Cains JH, Vilos AG. Fertility and pregnancy outcomes following resectoscopic septum division with and without intrauterine balloon stenting: a randomized pilot study. Ann Saudi Med 2013;33:34–9.
- Dabirashrafi H, Mohammad K, Moghadami-Tabrizi N, Zandinejad K, Moghadami-Tabrizi M. Is estrogen necessary after hysteroscopic incision of the uterine septum? J Am Assoc Gynecol Laparosc 1996;3:623–5.
- Nawroth F, Schmidt T, Freise C, Foth D, Romer T. Is it possible to recommend an "optimal" postoperative management after hysteroscopic metroplasty? A retrospective study with 52 infertile patients showing a septate uterus. Acta Obstet Gynecol Scand 2002;81:55–7.
- Tonguc EA, Var T, Yilmaz N, Batioglu S. Intrauterine device or estrogen treatment after hysteroscopic uterine septum resection. Int J Gynaecol Obstet 2010;109:226–9.
- Yu X, Yuhan L, Dongmei S, Enlan X, Tinchiu L. The incidence of post-operative adhesion following transection of uterine septum: a cohort study comparing three different adjuvant therapies. Eur J Obstet Gynecol Reprod Biol 2016;201:61–4.
- Chen H, Xiong W, Zeng Y, Du H, Ye L, Chen L, et al. Efficacy and safety of auto-cross-linked hyaluronic gel to prevent intrauterine adhesion after hysteroscopic electrosurgical resection: a multi-center randomized controlled trial. Ann Transl Med 2022;10:1217.
- Vandenberghe G, De Blaere M, Van Leeuw V, Roelens K, Englert Y, Hanssens M, et al. Nationwide population-based cohort study of uterine rupture in Belgium: results from the Belgian Obstetric Surveillance System. BMJ Open 2016;6:e010415.
- Candiani GB, Vercellini P, Fedele L, Carinelli SG, Merlo D, Arcaini L. Repair of the uterine cavity after hysteroscopic septal incision. Fertil Steril 1990;54:991–4.
- Berkkanoglu M, Isikoglu M, Arici F, Ozgur K. What is the best time to perform intracytoplasmic sperm injection/embryo transfer cycle after hysteroscopic surgery for an incomplete uterine septum? Fertil Steril 2008;90:2112–5.
Supplemental Table 1
| Authors | Title | Journal | QOE | Type | N= | Notes |
|
Agostini A, De Guibert F, Salari K, Crochet P, Bretelle F and Gamerre M |
Adverse obstetric outcomes at term after hysteroscopic metroplasty |
J Minim Invasive Gynecol 2009;16:454-7 |
Low |
Retrospective comparative (case-control) |
93 (62 control) |
|
|
Abu Rafea BF, Vilos GA, Oraif AM, Power SG, Cains JH and Vilos AG |
Fertility and pregnancy outcomes following resectoscopic septum division with and without intrauterine balloon stenting: a randomized pilot study |
Ann Saudi Med 2013;33:34-9 |
Intermediate |
Prospective RCT |
28 (15 control) |
data after 12 mon post metroplasty |
|
Bakas P, Gregoriou O, Hassiakos D, Liapis A, Creatsas M and Konidaris S |
Hysteroscopic resection of uterine septum and reproductive outcome in women with unexplained infertility |
Gynecol Obstet Invest 2012;73:321-5 |
Low |
Prospective observational |
68 |
first data pt, 12 mon follow up, then total (39 mon) |
|
Ban-Frangez H, Tomazevic T, Virant-Klun I, Verdenik I, Ribic-Pucelj M and Bokal EV |
The outcome of singleton pregnancies after IVF/ICSI in women before and after hysteroscopic resection of a uterine septum compared to normal controls |
Eur J Obstet Gynecol Reprod Biol 2009;146:184-7 |
Low |
Retrospective matched control |
411 (274 control) |
large uterine septum (Class V according to AFS classification; small partial (class VI) |
|
Bendifallah S, Faivre E, Legendre G, Deffieux X and Fernandez H |
Metroplasty for AFS Class V and VI septate uterus in patients with infertility or miscarriage: reproductive outcomes study |
J Minim Invasive Gynecol 2013;20:178-84 |
Low |
Retrospective observational |
128 |
rates of miscarriage & FLB signif different according to anatomical type of septum; FLB rate (7/128) |
|
Berkkanoglu M, Isikoglu M, Arici F and Ozgur K |
What is the best time to perform intracytoplasmic sperm injection/embryo transfer cycle after hysteroscopic surgery for an incomplete uterine septum? |
Fertil Steril 2008;90:2112-5 |
Low |
Retrospective cohort study |
282 |
incomplete uterine septum; all P values not signficant |
|
Bohlmann MK, Von Wolff M, Luedders DW, Beuter-Winkler P, Diedrich K, Hornemann A and Strowitzki T |
Hysteroscopic findings in women with two and with more than two first-trimester miscarriages are not significantly different |
Reprod Biomed Online 2010;21:230-6 |
Low |
Retrospective |
206 |
recurrent miscarriages (<14 wks completed) |
|
Bosteels J, Weyers S, Puttemans P, Panayotidis C, Van Herendael B, Gomel V, Mol BW, Mathieu C and D'hooghe T |
The effectiveness of hysteroscopy in improving pregnancy rates in subfertile women without other gynaecological symptoms: a systematic review |
Hum Reprod Update 2010;16:1-11 |
Intermediate |
Systematic Review of RCTs |
30 (papers) |
|
|
Cararach M, Penella J, Ubeda A and Labastida R |
Hysteroscopic incision of the septate uterus: scissors versus resectoscope |
Hum Reprod 1994;9:87-9 |
Low |
Prospective RCT |
81 |
(10/51) pregnancies in progress; PR by scissors better |
|
Colacurci N, De Franciscis P, Mollo A, Litta P, Perino A, Cobellis L and De Placido G |
Small-diameter hysteroscopy with Versapoint versus resectoscopy with a unipolar knife for the treatment of septate uterus: a prospective randomized study |
J Minim Invasive Gynecol 2007;14:622-7 |
Intermediate |
Prospective RCT |
160 (80 each group) |
|
|
Colacurci N, De Placido G, Perino A, Mencaglia L and Gubbini G |
Hysteroscopic metroplasty |
J Am Assoc Gynecol Laparosc 1998;5:171-4 |
Low |
Multicenter retrospective |
973 |
no difference in using diathermal loop vs laser vs scissors |
|
Dabirashrafi H, Mohammad K, Moghadami-Tabrizi N, Zandinejad K and Moghadami-Tabrizi M |
Is estrogen necessary after hysteroscopic incision of the uterine septum? |
J Am Assoc Gynecol Laparosc 1996;3:623-5 |
Low |
DM |
16 |
Tompkins technique used for metroplasty |
|
Dalal RJ, Pai HD, Palshetkar NP, Takhtani M, Pai RD and Saxena N |
Hysteroscopic metroplasty in women with primary infertility and septate uterus: reproductive performance after surgery |
J Reprod Med 2012;57:13-6 |
Low |
Prospective observational |
72 |
repeat surgery w/ women w/ septal remnant > 1 |
|
Daniilidis A, Kalpatsanidis A, Kalkan U, Kasmas S, Pados G and Angioni S |
Reproductive outcome after operative hysteroscopy for uterine septum: scissors or diathermy? |
Minerva Ginecol 2020;72:36-42 |
Intermediate |
Systematic review |
26 papers |
|
|
Detti L |
Ultrasound assessment of uterine cavity remodeling after surgical correction of subseptations |
Am J Obstet Gynecol 2014;210:262.e1-6 |
Low |
Prospective cohort |
28 (12 septate) |
|
|
Detti L, Hickman H, Levi D'ancona R, Wright AW and Christiansen ME |
Relevance of Uterine Subseptations: What Length Should Warrant Hysteroscopic Resection? |
J Ultrasound Med 2017;36:757-765 |
Intermediate |
Prospective controlled cohort |
153 (77 control) |
|
|
Di Spiezio Sardo A, Zizolfi B, Bettocchi S, Exacoustos C, Nocera C, Nazzaro G, Da Cunha Vieira M and Nappi C |
Accuracy of Hysteroscopic Metroplasty With the Combination of Presurgical 3-Dimensional Ultrasonography and a Novel Graduated Intrauterine Palpator: A Randomized Controlled Trial |
J Minim Invasive Gynecol 2016;23:557-66 |
High |
Prospective RCT |
90 (45 control) |
proportion of pts w/ complete septum resection significantly higher in group T (71.5% vs. 41%, p=0.006) |
|
Faivre E, Fernandez H, Deffieux X, Gervaise A, Frydman R and Levaillant JM |
Accuracy of three-dimensional ultrasonography in differential diagnosis of septate and bicornuate uterus compared with office hysteroscopy and pelvic magnetic resonance imaging |
J Minim Invasive Gynecol 2012;19:101-6 |
Intermediate |
Prospective cohort |
31 (20 septate) |
volume transvaginal 3-D ultrasonography extremely accurate |
|
Fedele L, Arcaini L, Parazzini F, Vercellini P and Di Nola G |
Reproductive prognosis after hysteroscopic metroplasty in 102 women: life-table analysis |
Fertil Steril 1993;59:768-72 |
Low |
Prospective cohort? |
102 (23 complete septate, 79 partial) |
at 36 months, cumulative PR = 89% |
|
Fedele L, Bianchi S, Marchini M, Mezzopane R, Di Nola G and Tozzi L |
Residual uterine septum of less than 1 cm after hysteroscopic metroplasty does not impair reproductive outcome |
Hum Reprod 1996;11:727-9 |
Intermediate |
Prospective |
72 (17 in 1st group) |
|
|
Freud A, Harlev A, Weintraub AY, Ohana E and Sheiner E |
Reproductive outcomes following uterine septum resection |
J Matern Fetal Neonatal Med 2015;28:2141-4 |
Low |
Retrospective cohort study |
28 |
increased rate of c-sections after resection (but NS) |
|
Ghirardi V, Bizzarri N, Remorgida V, Venturini PL and Ferrero S |
Intraoperative Transrectal Ultrasonography for Hysteroscopic Metroplasty: Feasibility and Safety |
J Minim Invasive Gynecol 2015;22:884-8 |
Low |
Prospective, comparative non-randomized study |
45 (18 control) |
|
|
Grynberg M, Gervaise A, Faivre E, Deffieux X, Frydman R and Fernandez H |
Treatment of twenty-two patients with complete uterine and vaginal septum |
J Minim Invasive Gynecol 2012;19:34-9 |
Low |
Retrospective |
22 |
fertility outcomes measured 2 yrs after |
|
Gundabattula SR, Joseph E, Marakani LR, Dasari S and Nirmalan PK |
Reproductive outcomes after resection of intrauterine septum |
J Obstet Gynaecol 2014;34:235-7 |
Low |
Retrospective |
124 |
post-resection PR of 75%, take home baby rate of 60%, outcomes only known for 85 out of 98 pregnancies post-resection |
|
Heinonen PK |
Complete septate uterus with longitudinal vaginal septum |
Fertil Steril 2006;85:700-5 |
Low |
Retrospective |
67 |
|
|
Imboden S, Müller M, Raio L, Mueller MD and Tutschek B |
Clinical significance of 3D ultrasound compared to MRI in uterine malformations |
Ultraschall Med 2014;35:440-4 |
Low |
Retrospectie analysis |
63 (group A=40 , group B=13, group C=10) |
3D-US most reliable diagnostic; paper translated from German by Google |
|
Jakiel G, Robak-Chołubek D and Przytuła-Piłat M |
Two-year studies of women with fertility problems following uterine septum hysteroscopic treatment |
Ann Univ Mariae Curie Sklodowska Med 2004;59:65-9 |
Low |
Retrospective |
31 |
|
|
Karadag B, Dilbaz B, Demir B, Ozgurluk I, Kocak M, Karasu Y, Gulsah Sahin E and Dilbaz S |
Reproductive performance after hysteroscopic metroplasty in infertile women: complete versus partial uterine septum |
Clin Exp Obstet Gynecol 2016;43:584-587 |
Low |
DM |
73 (32 complete) |
significant decrease in post-op miscarriage rates vs pre in both groups (p=0.001, p=0.001), also has reproductive outcomes comparing primary vs secondary infertility |
|
Kowalik CR, Goddijn M, Emanuel MH, Bongers MY, Spinder T, De Kruif JH, Mol BW and Heineman MJ |
Metroplasty versus expectant management for women with recurrent miscarriage and a septate uterus |
Cochrane Database Syst Rev 2011;Cd008576 |
High |
Review of RCTs |
0 studies |
no studies met their criteria |
|
Laganà AS, Ciancimino L, Mancuso A, Chiofalo B, Rizzo P and Triolo O |
3D sonohysterography vs hysteroscopy: a cross-sectional study for the evaluation of endouterine diseases |
Arch Gynecol Obstet 2014;290:1173-8 |
Low |
cross-sectional |
224 |
|
|
Litta P, Spiller E, Saccardi C, Ambrosini G, Caserta D and Cosmi E |
Resectoscope or Versapoint for hysteroscopic metroplasty |
Int J Gynaecol Obstet 2008;101:39-42 |
Low |
Prospective |
63 (21 resectoscope) |
|
|
Loddo A, D'alterio MN, Neri M, Masala F, Cane FL and Melis GB |
Pregnancy Complications After Hysteroscopic Metroplasty: A Ten-Year Case-Control Study |
Surg Technol Int 2017;30:205-209 |
Low/low |
|
|
|
|
Loverro G, Nappi L, Vicino M, Carriero C, Vimercati A and Selvaggi L |
Uterine cavity assessment in infertile women: comparison of transvaginal sonography and hysteroscopy |
Eur J Obstet Gynecol Reprod Biol 2001;100:67-71 |
Intermediate/intermediate |
Prospective |
134 |
hysteroscopy used as 2nd step if TVS gives doubtful results |
|
Ludwin A, Ludwin I, Kudla M, Pitynski K, Banas T, Jach R and Knafel A |
Diagnostic accuracy of three-dimensional sonohysterography compared with office hysteroscopy and its interrater/intrarater agreement in uterine cavity assessment after hysteroscopic metroplasty |
Fertil Steril 2014;101:1392-9 |
Intermediate/intermediate |
Prospective observational |
141 |
3D-SIS not signfiicantly different from hysteroscopy for diagnostic accuracy |
|
Ludwin A, Ludwin I, Pityński K, Banas T and Jach R |
Role of morphologic characteristics of the uterine septum in the prediction and prevention of abnormal healing outcomes after hysteroscopic metroplasty |
Hum Reprod 2014;29:1420-31 |
Intermediate/intermediate |
Prospective observational cohort |
96 (49 no barrier) |
|
|
Mollo A, De Franciscis P, Colacurci N, Cobellis L, Perino A, Venezia R, Alviggi C and De Placido G |
Hysteroscopic resection of the septum improves the pregnancy rate of women with unexplained infertility: a prospective controlled trial |
Fertil Steril 2009;91:2628-31 |
Intermediate/intermediate |
Prospective control |
176 (132 control) |
discrepency b/w abstract and methods regarding groups? |
|
Nawroth F, Schmidt T, Freise C, Foth D and Römer T |
Is it possible to recommend an "optimal" postoperative management after hysteroscopic metroplasty? A retrospective study with 52 infertile patients showing a septate uterus |
Acta Obstet Gynecol Scand 2002;81:55-7 |
Low/low |
Retrospective |
52 (group 1 = 22, group 2 = 13, group 3 = 13) |
|
|
Nouri K, Ott J, Huber JC, Fischer EM, Stögbauer L and Tempfer CB |
Reproductive outcome after hysteroscopic septoplasty in patients with septate uterus--a retrospective cohort study and systematic review of the literature |
Reprod Biol Endocrinol 2010;8:52 |
Low/low |
Retrospective cohort study, systematic review |
64 - cohort, 1501 - systematic review |
if interested, additional data about women w/ w/out history of miscarriage |
|
Ono S, Kuwabara Y, Matsuda S, Yonezawa M, Watanabe K, Akira S and Takeshita T |
Is hysteroscopic metroplasty using the incision method for septate uterus a risk factor for adverse obstetric outcomes? |
J Obstet Gynaecol Res 2019;45:634-639 |
Low/INTERMEDIATE |
Retrospective cohort |
1180 (1139 controls) |
incision method not risk factor for adverse obstetric outcomes |
|
Ozgur K, Bulut H, Berkkanoglu M and Coetzee K |
Perinatal outcomes in singleton and twin ICSI pregnancies following hysteroscopic correction of partial intrauterine septa |
J Assist Reprod Genet 2015;32:533-41 |
Intermediate/intermediate |
Retrospective observational |
2024 (1128, 566, 217, 113 respectively) |
preterm = <37 wks, very preterm = <32 weeks |
|
Ozgur K, Isikoglu M, Donmez L and Oehninger S |
Is hysteroscopic correction of an incomplete uterine septum justified prior to IVF? |
Reprod Biomed Online 2007;14:335-40 |
Intermediate/intermediate |
Retrospective |
235 (group 1 = 119, group 2 = 116) |
|
|
Pabuçcu R and Gomel V |
Reproductive outcome after hysteroscopic metroplasty in women with septate uterus and otherwise unexplained infertility |
Fertil Steril 2004;81:1675-8 |
Low/low |
Prospective observational |
61 |
|
|
Paradisi R, Barzanti R, Natali F, Guerrini M, Battaglia C, Seracchioli R and Venturoli S |
Hysteroscopic metroplasty: reproductive outcome in relation to septum size |
Arch Gynecol Obstet 2014;289:671-6 |
Intermediate/LOW |
Retrospective and comparative cohort |
112 |
2.5cm cutoff arbitrarily selected based on uterine cavity size |
|
Parsanezhad ME, Alborzi S, Zarei A, Dehbashi S, Shirazi LG, Rajaeefard A and Schmidt EH |
Hysteroscopic metroplasty of the complete uterine septum, duplicate cervix, and vaginal septum |
Fertil Steril 2006;85:1473-7 |
Intermediate/intermediate |
Multicenter RCT |
28 (15 group A) |
|
|
Porcu G, Cravello L, D'ercole C, Cohen D, Roger V, De Montgolfier R and Blanc B |
Hysteroscopic metroplasty for septate uterus and repetitive abortions: reproductive outcome |
Eur J Obstet Gynecol Reprod Biol 2000;88:81-4 |
Low/low |
Retrospective |
63 |
|
|
Rikken JF, Kowalik CR, Emanuel MH, Mol BW, Van Der Veen F, Van Wely M and Goddijn M |
Septum resection for women of reproductive age with a septate uterus |
Cochrane Database Syst Rev 2017;1:Cd008576 |
Intermediate |
Retrospective observational, systematic review |
DM |
no RCTs found, aka search resulted in 0 papers |
|
Saygili-Yilmaz E, Yildiz S, Erman-Akar M, Akyuz G and Yilmaz Z |
Reproductive outcome of septate uterus after hysteroscopic metroplasty |
Arch Gynecol Obstet 2003;268:289-92 |
Low/low |
Retrospective |
361 (case 1 = 193, case 2 = 109, case 3 = 59) |
p<0.001 comparing pregnancy probability of 3 groups, IUD inserted post pro-cedure to reduce adhesion formation |
|
Sendag F, Mermer T, Yucebilgin S, Oztekin K and Bilgin O |
Reproductive outcomes after hysteroscopic metroplasty for uterine septum |
Clin Exp Obstet Gynecol 2010;37:287-9 |
Lowlow |
Retrospective |
30 |
|
|
Shokeir T, Abdelshaheed M, El-Shafie M, Sherif L and Badawy A |
Determinants of fertility and reproductive success after hysteroscopic septoplasty for women with unexplained primary infertility: a prospective analysis of 88 cases |
Eur J Obstet Gynecol Reprod Biol 2011;155:54-7 |
Lowlow |
Prospective comparative observational |
103 |
PR significantly higher for women <35 vs > and unexplained infertility for <3 years v > (p<0.001); PR NS w/ septum size |
|
Smit JG, Kasius JC, Eijkemans MJ, Veersema S, Fatemi HM, Santbrink Van EJ, Campo R and Broekmans FJ |
The international agreement study on the diagnosis of the septate uterus at office hysteroscopy in infertile patients |
Fertil Steril 2013;99:2108-13.e2 |
Low/low |
Interobserver |
78 |
*reproducibility study -> diagnosis agreement when fundal bulging present; no consensus on uterine shape; variation by country |
|
Smit JG, Overdijkink S, Mol BW, Kasius JC, Torrance HL, Eijkemans MJ, Bongers M, Emanuel MH, Vleugels M and Broekmans FJ |
The impact of diagnostic criteria on the reproducibility of the hysteroscopic diagnosis of the septate uterus: a randomized controlled trial |
Hum Reprod 2015;30:1323-30 |
Intermediate/intermediate |
RCT |
191 (105 control) |
septate diagnosis 0.59 vs. 0.52 (in non-instruction group); p=0.002; once diagnosed, agreement on the need for surgery poor |
|
Sparac V, Kupesic S, Ilijas M, Zodan T and Kurjak A |
Histologic architecture and vascularization of hysteroscopically excised intrauterine septa |
J Am Assoc Gynecol Laparosc 2001;8:111-6 |
Low/low |
Prospective consecutive |
76 |
septa consist of same tissue type as normal myometrium |
|
Şükür YE, Yakıştıran B, Özmen B, Sönmezer M, Berker B and Atabekoğlu C |
Hysteroscopic Corrections for Complete Septate and T-Shaped Uteri Have Similar Surgical and Reproductive Outcome |
Reprod Sci 2018;25:1649-1654 |
Low/low |
Retrospective cohort |
174 (97 complete) |
operating time for t-shaped significantly shorter, no difference in intraoperative/post-op complications |
|
Tomazevic T, Ban-Frangez H, Ribic-Pucelj M, Premru-Srsen T and Verdenik I |
Small uterine septum is an important risk variable for preterm birth |
Eur J Obstet Gynecol Reprod Biol 2007;135:154-7 |
Low/low |
Observational |
730 |
826 total deliveries; group A - 112 before, 294 after; group b - 107 before, 313 after |
|
Tomaževič T, Ban-Frangež H, Virant-Klun I, Verdenik I, Požlep B and Vrtačnik-Bokal E |
Septate, subseptate and arcuate uterus decrease pregnancy and live birth rates in IVF/ICSI |
Reprod Biomed Online 2010;21:700-5 |
Low/low |
Retrospective matched control |
2481 embryo transfers |
# and quality of embryos transferred (2-3 vs 1), absence of uterine septum significantly influenced pregnancy rate (p=.034, p<0.001, p<0.001 respectively) |
|
Tonguc EA, Var T and Batioglu S |
Hysteroscopic metroplasty in patients with a uterine septum and otherwise unexplained infertility |
Int J Gynaecol Obstet 2011;113:128-30 |
Low/low |
Retrospective RCT? |
127 (25 group 2, control) |
|
|
Tonguc EA, Var T, Yilmaz N and Batioglu S |
Intrauterine device or estrogen treatment after hysteroscopic uterine septum resection |
Int J Gynaecol Obstet 2010;109:226-9 |
Low/low |
Prospective |
79 (19 control, group 2= 16, group = 19, group 4=25 |
neither IUD placement nor estrogen treatment prevent intrauterine adhesions or facilitate pregnancy (all data NS) |
|
Valli E, Vaquero E, Lazzarin N, Caserta D, Marconi D and Zupi E |
Hysteroscopic metroplasty improves gestational outcome in women with recurrent spontaneous abortion |
J Am Assoc Gynecol Laparosc 2004;11:240-4 |
Low/low |
prospective |
48 (15 controls) |
*note data is from first pregnancy after enrollment (table also had 'all pregnancies') |
|
Valli E, Zupi E, Marconi D, Vaquero E, Giovannini P, Lazzarin N and Romanini C |
Hysteroscopic findings in 344 women with recurrent spontaneous abortion |
J Am Assoc Gynecol Laparosc 2001;8:398-401 |
Low |
Retrospective |
1,266 (922 controls) |
significant difference (p<0.01) b/w RSA (30/344) and control group (17/922) for septate |
|
Vandenberghe G, De Blaere M, Van Leeuw V, Roelens K, Englert Y, Hanssens M and Verstraelen H |
Nationwide population-based cohort study of uterine rupture in Belgium: results from the Belgian Obstetric Surveillance System |
BMJ Open 2016;6:e010415 |
Low/low |
Population-based prospective cohort |
90 |
comparable to other Western countries; 2 cases followed uterine septum resection |
|
Venetis CA, Papadopoulos SP, Campo R, Gordts S, Tarlatzis BC and Grimbizis GF |
Clinical implications of congenital uterine anomalies: a meta-analysis of comparative studies |
Reprod Biomed Online 2014;29:665-83 |
Intermediate/intermediate |
Systematic review and meta-analysis |
25 studies |
only looked at comparative studies, most data was risk ratio, about congenital uterine anomalies IN GENERAL |
|
Wang X, Hou H and Yu Q |
Fertility and pregnancy outcomes following hysteroscopic metroplasty of different sized uterine septa: A retrospective cohort study protocol |
Medicine (Baltimore) 2019;98:e16623 |
Low/low |
Retrospective cohort study |
121 (group A=35, group B=48, group C=48) |
|
|
Wang Z, An J, Su Y, Liu C, Lin S, Zhang J and Xie X |
Reproductive outcome of a complete septate uterus after hysteroscopic metroplasty |
J Int Med Res 2020;48:300060519893836 |
Low/low |
Prospective screening |
1089 (normal=983, arcuate=72, subseptate=29 |
subseptate uterus significantly higher proportion of first-trimester losses (p<0.1) |
|
Yu X, Yuhan L, Dongmei S, Enlan X and Tinchiu L |
The incidence of post-operative adhesion following transection of uterine septum: a cohort study comparing three different adjuvant therapies |
Eur J Obstet Gynecol Reprod Biol 2016;201:61-4 |
Intermediate/intermediate |
Retrospective cohort |
238 (group 1= 50, group 2=59, group 3=75, group 4=54) |
no significant difference in adhesions b/w groups |
|
Zlopasa G, Skrablin S, Kalafatić D, Banović V and Lesin J |
Uterine anomalies and pregnancy outcome following resectoscope metroplasty |
Int J Gynaecol Obstet 2007;98:129-33 |
Low |
Observational |
25 |
also data comparing reproductive outcomes in women w/ uterine anomalies vs normal; poorest fetal survival found w/ subseptate & septate subgroups |
Practice Documents
ASRM Practice Documents have been developed to assist physicians with clinical decisions regarding the care of their patients.
Fertility preservation in patients with medical indications: a committee opinion (2026)
Expert guidelines on fertility preservation options—oocyte, embryo, ovarian and testicular tissue cryopreservation and counseling before gonadotoxic treatment.
The reproductive endocrinology and infertility subspecialist: definition, training, and scope of practice in the United States (2025)
Reproductive endocrinology and infertility (REI) subspecialists are physicians with extensive and specialized training in the diagnosis and treatment of complex reproductive disorders.
Improving access to care and delivery to marginalized and vulnerable populations: a committee opinion (2025)
ASRM committee opinion on reducing infertility care disparities, outlining barriers and actionable strategies to improve equitable access.
Evidence-based guideline: Premature Ovarian Insufficiency (2025)
This guideline on premature ovarian insufficiency (POI) offers best practice advice on the care of women with POI.More Resources
ASRM Practice Documents

ASRM MAC Tool 2021
The ASRM Müllerian Anomaly Classification 2021 (MAC2021) includes cervical and vaginal anomalies and standardize terminology within an interactive tool format.

Coding Corner Q & A
The Coding Corner Q & A is a list of previously submitted and answered questions from ASRM members about coding. Answers are available to ASRM Members only.

EMR Shared Phrases/Template Library
This resource includes phrases shared by ASRM physician members to provide a template for individuals to create their own EMR phrases.

ASRM Ethics Opinions
Ethics Committee Reports are drafted by the members of the ASRM Ethics Committee on the tough ethical dilemmas of reproductive medicine.

COVID-19 Resources
A compendium of ASRM resources concerning the Novel Corona virus (SARS-COV-2) and COVID-19.

Patient Resources
ReproductiveFacts.org provides a wide range of information related to reproductive health and infertility through patient education fact sheets, infographics, videos, and other resources.
Topic Resources
Same Day Consult and Procedure
I saw a patient for consultation who had irregular uterine bleeding. View the AnswerHysteroscopy Polyp Suspected
What ICD-10 code do you use if a diagnostic hysteroscopy is performed for the preoperative diagnosis of uterine polyp? View the AnswerTopic Resources
SRS Travel Scholar Award for Reproductive Surgery
The objective of the SRS Traveling Scholar Award is to provide for any trainee whose abstract submission focuses on reproductive surgery to expand their educational and networking experience. View the Award InformationSRS-SMRU Travel Scholar Award for Male Reproductive Surgery
The objective of the SRS-SMRU Traveling Scholars Award is for any trainee whose abstract submission focuses on male reproductive surgery to expand their educational and networking experience. View the Award InformationSRS In-Training Awards for Research
DeCherney-Nezhat REI Fellows Traveling Scholars Award in Reproductive Surgery
The objective of this award is to expand educational and networking opportunities for REI Fellows with a focus on reproductive surgery. View the Award InformationFertility and Sterility On Air - Live from the American Association of Gynecologic Laparoscopists 2025 Global Congress
Expert surgeons and REIs explore cutting-edge adenomyosis diagnosis and treatment to improve fertility outcomes, live from AAGL-ASRM. Listen to the EpisodeHow to Code for Surgical Tubal Anastomosis
How do you properly code this surgical tubal anastomosis and chromotubation? In this case, codes 58679 and 58662 were billed View the AnswerASRM Hosts Capitol Hill Briefing for Policymakers & Congressional Staff to Hear From Providers & Patients About Importance of IVF Access, Realities and Limitations of Restorative Reproductive Medicine
ASRM briefing united lawmakers, physicians & patients on IVF access, exposing RRM limits and urging policies to expand fertility care options. View the Press ReleaseSRS Warns Against Limiting Access to IVF Under the Guise of “Restorative” Care
SRS, an ASRM affiliate, advocates evidence-based reproductive surgery and full-spectrum fertility care for conditions like endometriosis, fibroids, and PCOS. View the Press ReleaseReimplantation of cryopreserved ovarian tissue
What is the correct code for laparoscopic reimplantation of ovarian tissue? View the AnswerCoding for fluid aspiration during HSG
For physician-performed sonoHSG (58340& 76831) and uterine aspiration due to fluid, can an additional code for the aspiration be billed? View the AnswerBilling 58558 together with 58560
Can CPT codes 58558 and 58560 be billed together? Also, can 58560 be billed with place of service 11? View the AnswerCoding of identification of sperm in aspirate
During vasovasostomy/vasoepididyostomy procedures, our surgeons perform intra-op sperm identification from aspirate View the AnswerSurgical Options for Fertility Care
Dr. Zaraq Khan discusses his journey and passion for reproductive surgery, addressing complex fertility challenges and advocating for better surgical training and research. View the ASRMed Talk VideoEndometrioma
Surgery was performed under anesthesia for Aspiration of right hyrosalpinx fluid and right endometrioma. View the AnswerUterine Aspiration of Pregnancy of Unknown Location
What CPT code would be most appropriate for a manual uterine aspiration for a pregnancy of unknown location? View the AnswerEligibility to bill for facility fee
We are planning to open a new fertility clinic and I was wondering about the eligibility to bill insurance companies for “facility fee” for egg retrievals. View the AnswerResection Adenomyoma
I have a patient with an adenomyoma of the uterine wall that requires surgical excision and uterine repair. View the AnswerRobotically Assisted Tubal Anastomosis
What is the correct CPT code for laparoscopic tubal anastomosis with robotic assistance? View the AnswerSurgery Coding
I took the ASRM coding course, and in that course, coding for bilateral neosalpingostomies was coded using only a dx of N70.11 (hydrosalpinx). View the AnswerTompkins Metroplasty
Is there a code for Tompkins Metroplasty? View the AnswerMultiple Laparoscopic Procedures
Is it appropriate to bill for medically indicated, multiple procedures when performing laparoscopies? View the AnswerOffice Hysteroscopy Billing
Do you all have a resource that details what all can be billed, or what all is bundled with the 58558 procedure when done in office? View the AnswerOvarian Drilling
Is there a CPT Code for "Ovarian Drilling"? View the AnswerOvariopexy
Learn how to code ovariopexy for benign disease via mini-laparotomy, including CPT options like 49000 with modifier 22 or 58999 for unlisted procedures. View the AnswerExcision Ovarian Endometrioma
What code is used for a laparoscopic excision of endometriosis and an ovarian excision of endometrioma with bilateral ureterolysis is performed. View the AnswerHysteroscopic Tubal Cannulation Under Laparoscopic Guidance
How can one code for hysteroscopic transcervical fallopian tube cannulation under laparoscopic guidance? View the AnswerHysteroscopy Polyp Suspected
What ICD-10 code do you use if a diagnostic hysteroscopy is performed for the preoperative diagnosis of uterine polyp? View the AnswerHysteroscopy Recurrent Implantation Failure
What is the appropriate ICD-10 code for recurrent implantation failure? View the AnswerHysteroscopy Resection of Retained Products of Conception
What CPT is appropriate for a Hysteroscopy Resection of Retained Products of Conception? View the AnswerD&C Under Ultrasound Guidance
What are the CPT codes and ICD-10 codes for coding a surgical case for a patient with history of Stage B adenocarcinoma of the cervix ... View the AnswerDiagnostic Hysteroscopy
If the doctors do a hysteroscope #58555 in the office with a Endosee Scope, can I still use the same code even though it is in the office? View the AnswerC-Section Ectopic Pregnancy
I’m writing for advice for CPT advice for managing cesarean scar ectopic pregnancy without concurrent intrauterine pregnancy (ICD-10 O00.80). View the AnswerCoding for Ovarian Drilling
Can you provide some information related to ovarian drilling that would assist non-physician administration (coders, billers)? View the AnswerCoding For Placement Of A Cervical Stitch
Physicians at our practice are placing a stitch and dilating the cervix after egg retrievals for those patients that have cervical stenosis. View the AnswerCycle Monitoring Fertility Preservation
If the patient is undergoing ultrasound tracking visits for fertility preservation, what I ICD-10 code do you use for the monitoring? View the AnswerJournal Club Global: Moving leiomyoma research from bench to bedside
Role of tubal surgery in the era of assisted reproductive technology: a committee opinion (2021)
This document reviews surgical options for reparative tubal surgery and the factors that must be considered when deciding between surgical repair and IVF.View the Committee Opinion